Article Text

Abstract
Background: Randomised trials have demonstrated that the efficacy of anti-tumour necrosis factor (TNF) agents is significantly increased by concomitant methotrexate (MTX) in rheumatoid arthritis (RA). In clinical routine, anti-TNF agents are commonly prescribed with other disease-modifying antirheumatic drugs (DMARDs) than MTX, however their effectiveness in combination with anti-TNF agents is not well established.
Objective: To compare the effectiveness of leflunomide (LEF) and other conventional DMARDs with MTX as co-therapy to anti-TNF agents in RA.
Methods: All patients on anti-TNF agents and conventional DMARDs within the Swiss Clinical Quality Management (SCQM)-RA database were included (n = 1218) and categorised according to the type of co-therapy into anti-TNF+MTX (n = 842), anti-TNF+LEF (n = 260) and anti-TNF+other DMARDs (n = 116). Drug discontinuation rates and incidence of toxic side effects were analysed using Cox proportional hazard models. Progression of radiographic damage, the evolution of functional disability and the improvement of RA disease activity were analysed using longitudinal regression models, adjusting for potential confounders.
Results: The overall discontinuation rates of anti-TNF and conventional DMARD combination therapies were relatively high with a median survival of only 16 months (interquartile range (IQR): 10–37), but they did not differ between the three regimens (p = 0.69). The progression of radiographic damage (p = 0.77), functional disability (p = 0.09) and RA disease activity (p = 0.33) were also similar between the different regimen. In addition, no significant difference in the frequency of adverse events emerged.
Conclusion: Overall these results suggest that LEF and potentially other conventional DMARDs offer an effective and safe alternative to MTX as co-therapy in combination with anti-TNF agents.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease that leads to progressive joint destruction, functional disability and extra-articular complications. New biological disease-modifying antirheumatic drugs (DMARDs) became available in 1999, including agents targeting tumour necrosis factor α (anti-TNF agents). Among these, infliximab (INF), etanercept (ETN) and adalimumab (ADA) have been shown to reduce signs and symptoms of RA and to protect joints from structural damage in double-blind placebo-controlled randomised controlled trials (RCT). Certain anti-TNF agents can be prescribed alone, but randomised trials have consistently demonstrated that the efficacy of these biological agents is significantly increased by concomitant methotrexate (MTX).1 However, not all patients tolerate or respond to MTX, and anti-TNF agents are commonly prescribed with other DMARDs than MTX in clinical routine.2 Nevertheless, the effectiveness of non-MTX DMARDs as co-therapy with anti-TNF agents is not well established. The efficacy and safety of the combination of ETN and sulphasalazine as compared to either drug alone has been reported in a RCT of patients with incomplete response to sulphasalazine. The results demonstrated that the efficacy was similar in both groups treated with ETN, but superior to patients receiving sulphasalazine alone3 Safety data were not significantly different in patients treated with the combination as compared to ETN alone.
One of the most commonly prescribed concomitant DMARD with anti-TNF agents is leflunomide (LEF).4 LEF is a pyrimidine synthesis inhibitor with immunomodulatory properties and anti-inflammatory activity, which has demonstrated its efficacy as a DMARD.5 Several smaller retrospective case series have concluded that LEF in combination with anti-TNF agents appears to be effective and safe with appropriate monitoring.6–10 Prospective case series and cohort studies have generally confirmed the efficacy of this combination.11–13 By contrast, a short clinical trial of adalimumab and conventional DMARDs suggested that the efficacy of the combination with LEF was slightly lower than the combination with MTX, and the incidence of serious adverse events slightly higher.14 15 Overall, there is currently no evidence from controlled trials that anti-TNF combinations with LEF are as effective as anti-TNF combinations with MTX. The objective of this study was therefore to compare retention rates, effectiveness and safety of therapeutic regimen associating anti-TNF agents and LEF, MTX or other conventional DMARDs in a large population-based RA cohort.
PATIENTS AND METHODS
Study population
Regulatory authorities in Switzerland have recommended continuous monitoring of all patients receiving biological agents for arthritides and selected the Swiss Clinical Quality Management (SCQM) system to follow patients with RA treated with anti-TNF agents.16 Patients are generally enrolled prior to the initiation of anti-TNF therapy. The SCQM system mandates annual measurements of disease activity, radiographic damage, side effects and various symptom questionnaires.16 Clinical information is updated every time the patient’s disease status requires a change in their antirheumatic therapy. The patient’s rheumatologist or primary care doctor are incited to enrol their patient in the SCQM by allowing them to deduct costs of anti-TNF drugs from their global treatment expenditure, scrutinised by the health authorities, which contributes to a high enrolment rate.17 Patients come from a range of clinical settings with 50% from private practices, 25% non-academic centres and 25% academic centres. The accuracy of medication data provided by the doctors, including anti-TNF start and stop dates, was confirmed against participants’ self-reported information and an additional assessment with the treating rheumatologist.
Study design
This is a longitudinal observational study of a population-based cohort of patients with RA. The analysis included data collected from March 1996 to December 2006. The inclusion criteria included a diagnosis of RA by a rheumatologist and treatment with INF, ETN or ADA. The exclusion criteria were the absence of concomitant DMARD therapy, and the simultaneous prescription of LEF and MTX in combination with anti-TNF agents, because the primary objective of this study was to study patients on LEF, MTX or other DMARDs.
Outcomes
We considered four outcomes that operationally define effectiveness: the overall retention rate of the current combination of anti-TNF agents and conventional DMARDs, the progression of long-term radiographic damage, the evolution of functional disability, and the improvement of RA disease activity.
We examined drug retention of current combination of anti-TNF agents and conventional DMARDs using the time until drug discontinuation, independently of the reason that led to drug interruption. Drug discontinuation rates or “drug survival rates” reflect patient and doctor satisfaction with a given therapy, and thus represent a useful summary measure of the overall treatment effectiveness and tolerability.18 19 Drug interruption was defined as the discontinuation of the current therapeutic combination, ie, the interruption of either the anti-TNF agent or the concomitant DMARD, or both. Temporary interruptions (less than 6 months) were not considered a discontinuation, neither were treatment interruptions for remission.
A second end point was the progression of radiographic joint damage as measured by changes from baseline in radiographic damage scores. Radiographic damage was assessed prospectively by a single assessor on serial radiographs with a validated scoring system (Ratingen Score) according to a previously published method.20 The scoring method is sensitive to change and less susceptible to ceiling effects in advanced disease because of a true ordinal rating scheme.21 The reliability of this scoring method is excellent, with an intraclass correlation coefficient (ICC) for intra-rater reliability of 0.8 to 0.9 and an ICC for inter-rater reliability of 0.7 to 0.9.13 20 The minimal detectable radiographic change for this method has been determined to be 3.3% of the maximum score.20 The intra-rater reliability for the study assessor of these radiographs was good, with an intraclass correlation coefficient (ICC) of 0.94 for a cross-sectional assessment and an ICC of 0.71 for change scores. Sporadic missing joints in follow-up radiographs due to poor positioning were scored conservatively as unchanged using the “last observation carried forward” procedure.
Another outcome of this study was the progression of functional disability as measured by change from baseline in the Stanford Health Assessment Questionnaire disability index (HAQ) (10). The HAQ is a 20-item self-report questionnaire ranging from 0 to 3, which tends to increase in score slowly over time in RA (average of 0.03 units per year).22 The HAQ is the most widely used functional status questionnaire in rheumatology and has been shown to predict work disability,23 joint replacement,23 medical costs24 and mortality25 in RA.
Finally, we examined RA disease activity using the Disease Activity Score in 28 joints (DAS28).26 The DAS28 is a validated doctor assessment of disease activity in RA, which includes number of swollen joints, the number of tender joints and the erythrocyte sedimentation rate.26 The DAS28 score ranges from 0 to 9.2, where 9.2 represents maximum disease activity.
A secondary outcome was the tolerability and side effect profile of the conventional DMARD co-therapies. Other important predictors of RA disease progression such self-assessed symptom questionnaires, various disease characteristics, and demographic characteristics were extracted from the database to be used in the analysis.
Exposure variables
The exposure of interest for this study was the type of conventional DMARD used in combination with anti-TNF agents. All patients treated with anti-TNF were thus categorised as MTX co-therapy (aTNF+MTX), LEF co-therapy (aTNF+LEF), or other DMARD co-therapy (aTNF+other DMARD). Other DMARD co-therapy included sulphasalazine, hydroxychloroquine, minocycline, azathioprine, cyclosporine A, d-penicillamine, oral or intramuscular gold salts. Concomitant glucocorticoid intake was considered separately. We excluded a priori patients on anti-TNF agents without conventional DMARD co-therapy, because it is well established that anti-TNF therapy is more effective in combination with these agents;1 2 therefore it is likely that patients on anti-TNF monotherapy have a more benign form of the disease or a history of more adverse reactions on conventional DMARDs, which might have biased the results if included (selection bias).
Analysis
Baseline disease characteristics were compared between the three treatment strategies. The significance of differences in mean values of continuous variables was assessed with one-way analysis of variance (ANOVA) for normally distributed variables and with the Kruskal–Wallis test for non-normally distributed variables. For dichotomous variables, the Pearson χ2 test was used to evaluate the statistical significance of differences in proportions. All statistical tests were two-sided and evaluated at the 0.05 significance level. The statistical analysis was performed with Stata V.9.2 (Stata Statistical Software, College Station, Texas, USA).
Confounding was a concern in this study, because the choice of DMARD co-therapy could be associated with disease severity or treatment tolerability. Because such an association may substantially influence disease progression, we used multivariate adjustments to overcome such confounding effects. The time to discontinuation of anti-TNF combination regimen was analysed using a Cox proportional hazards model.27 Survival curves of the time to discontinuation (“drug survival”) were produced with the Kaplan–Meier product-limit method.27 Radiographic damage, functional disability and RA disease activity evolution were analysed using generalised mixed models for longitudinal data.28 We first selected the best fitting model without controlling for potential confounders (crude model). We verified that the multivariate normal assumption for longitudinal models was satisfied and examined whether time as a linear trend or as a polynomial function fit the data best. We then adjusted the analysis for differences in baseline disease characteristics. Rheumatoid factor, age, sex, disease duration, number of previous DMARDs, type of anti-TNF agent and previous anti-TNF failure were all considered confounders a priori and added into the model. We tested other covariates using a backwards stepwise selection approach. The final model was adjusted for differences in disease activity (DAS28), functional disability (HAQ), glucocorticoid use, presence of rheumatoid factor, gender, age, disease duration, number of previous DMARD, type of anti-TNF agent and previous anti-TNF failure. Point estimates of the regression model were used to produce the result graphs. Pairwise comparisons between the three treatment groups were planned a priori, but were considered only if the overall comparison indicated a significant difference (ANOVA, p<0.05). To maintain a type I error at 5%, pairwise comparisons and confidence intervals of therapeutic groups were corrected with the Bonferroni adjustment procedure.
RESULTS
A total of 1218 patients with RA met the study inclusion criteria out of a total 2097 patients in the SCQM databank given anti-TNF agents. We excluded patients on anti-TNF agents alone without concomitant DMARDs (843 patients) in order to minimise potential selection biases. We further excluded 36 patients who simultaneously received MTX, LEF and an anti-TNF agent. The 1218 patients had an average of three follow-up assessments (interquartile range (IQR): 2–4) and a follow-up period of 17 months. The majority of patients used MTX as co-therapy with anti-TNF agents (n = 842, 69%); the second most common conventional DMARD used in combination with anti-TNF agents was LEF (n = 260, 21%); other conventional DMARDs were prescribed infrequently (n = 116, 10%). The median dose of MTX at baseline was 15 mg/week (IQR: 10–20 mg/week) and the median dose of LEF at baseline was 20 mg/day (IQR (20–20 mg/day). The other conventional DMARD group was comprised of sulphasalzine (n = 37, 32%), azathioprine (n = 28, 24%), hydroxychloroquine (n = 21, 18%), cyclosporine (n = 7, 6%), injectable gold salts (n = 4, 3%), penicillamine (n = 3, 3%) and combinations of the above (n = 16, 14%). No significant differences were found for baseline disease characteristics between treatment groups (table 1). However, treatment characteristics differed somewhat between these groups, with, for example, MTX being combined more commonly with INF than with other anti-TNF agents (36% versus 27%, p = 0.01) and LEF and other DMARDs having a history of more prior failures on conventional DMARDs than MTX (median of 2 versus 1, p<0.001). Furthermore, low dose glucocorticoids were used more frequently in combination in the other DMARD group compared to the MTX and LEF groups (67% versus 48–51%, p>0.001).
Discontinuation of therapy
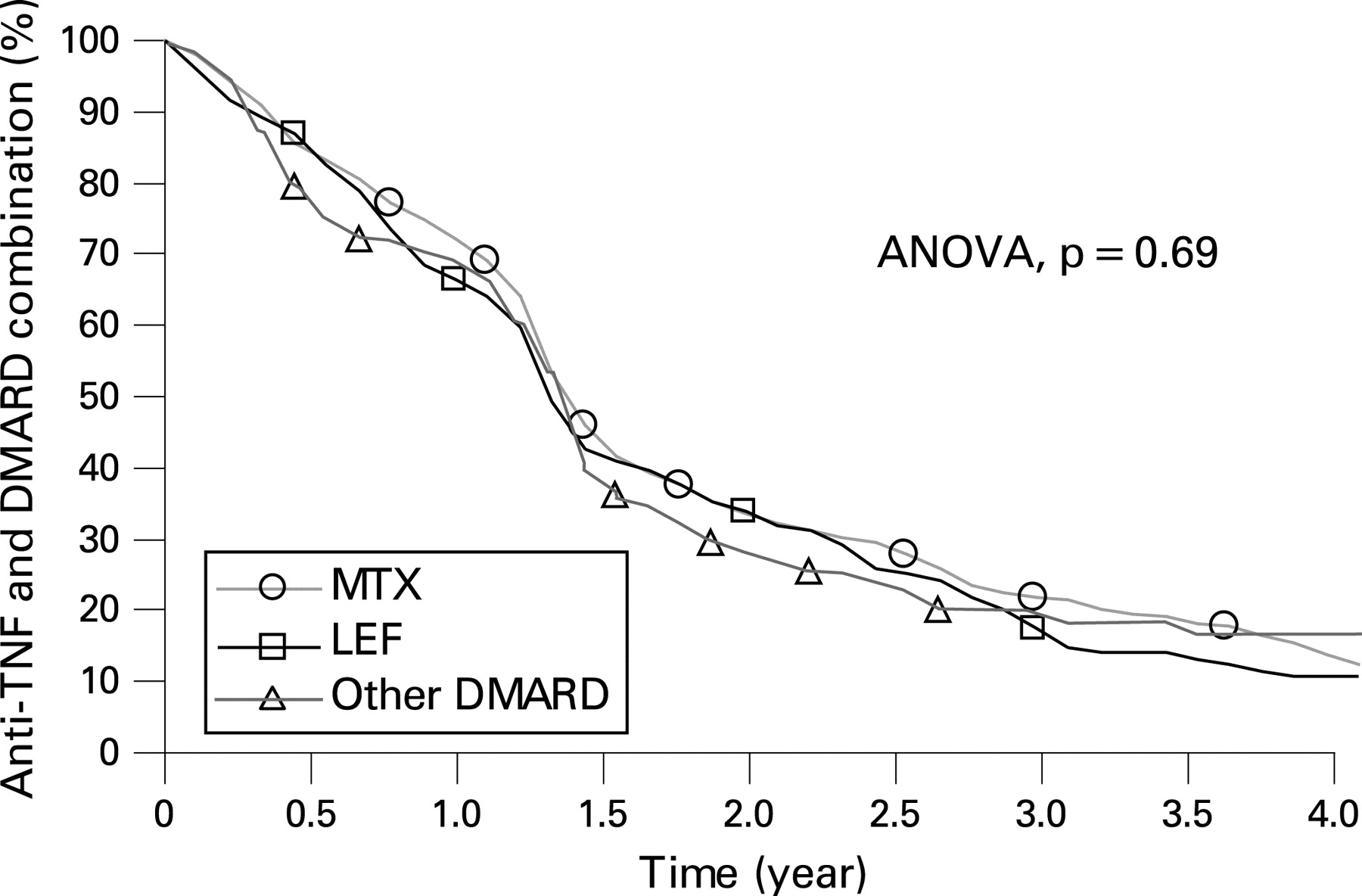
The discontinuation rates did not differ significantly between the three combinations of conventional DMARDs and anti-TNF agents (adjusted ANOVA, p = 0.69) (fig 1). A total of 1410 patient-years of combination therapy and 629 cases of treatment interruption were examined. The overall discontinuation rate of these combinations was relatively high, with a median survival of only 16 months (IQR: 10–37), which is significantly higher than the discontinuation rate of the individual anti-TNF agents (median survival 31.5 months (IQR: 12–68). The adjusted hazard ratio (HR) of discontinuing therapy was 1.08 (99% confidence interval (CI): 0.82–1.42) for the combination of LEF and anti-TNF agents compared to the other combinations, 0.92 (99% CI: 0.72–1.17) for MTX, and 1.06 (99% CI: 0.71–1.59) for other DMARDs. The unadjusted Cox proportional hazard model did display a lower discontinuation rate for the combination of anti-TNF and MTX (HR 0.79, 99% CI 0.63–0.99, crude ANOVA: p = 0.02), which completely disappeared when adjusted for the number of prior DMARDs and prior failures with anti-TNF agents, suggesting that these variables partially confounded the crude results. As expected, prior failure on another anti-TNF agent increased the rate of drug discontinuation (HR: 1.74, 95% CI: 1.59–1.90). Other significant predictors of discontinuation were increased disease activity at baseline as measured by the DAS28 (HR: 1.09, 95% CI: 1.03–1.16) and shorter disease durations (HR: = 0.98, 95% CI: 0.97–0.99).

Therapeutic effectiveness on RA disease progression
We did not find significant differences between the three combinations of conventional DMARDs and anti-TNF in radiographic damage progression (adjusted ANOVA: p = 0.77, fig 2A), functional disability progression (HAQ) (adjusted ANOVA: p = 0.09, fig 2B), or evolution of RA disease activity (DAS28) over time (adjusted ANOVA: p = 0.33, fig 2C). The unadjusted analyses displayed very similar results.

{kind=link}
{kind=link}
Overall, radiographic damage progressed only insignificantly with all three therapeutic combinations (fig 2A): Patients on anti-TNF+MTX progressed on average by 0.91% (99% CI: 0.54–1.27), patients on anti-TNF+LEF by 0.74% (99% CI: 0.21–1.27) and patients on anti-TNF+other DMARDs by 0.71% (99% CI: −0.02–1.44) of the maximum possible erosion score at 1 year. Significant predictors for increased radiographic progression were elevated functional disability at baseline as measured by the HAQ (p<0.001), recent disease onset (p<0.001), older age (p = 0.004) and numerous failures on previous DMARDs (p<0.001).
Functional disability generally improved during the first and second year after initiation of the combination of anti-TNF agents and conventional DMARDs (fig 2B) and the therapeutic response was similar with all three combinations. After 1 year, HAQ scores improved by 0.12 (99% CI: 0.08–0.15) with anti-TNF+MTX, by 0.14 (99% CI: 0.07–0.20) with anti-TNF+LEF, and by 0.13 (99% CI: 0.03–0.23) with anti-TNF+other DMARDs. Significant predictors for functional disability improvement were younger age (p<0.001), male gender (p<0.001), recent disease onset (p<0.001), lower disease activity at baseline as measured by the DAS28 (p<0.001), less failures on previous DMARDs (p<0.001) and no need for concomitant glucocorticoids (p<0.001).
The level of improvement in disease activity also varied little between the three groups: DAS28 improved by 0.74 (99% CI: 0.63–0.84) with anti-TNF+MTX, by 0.63 (99% CI: 0.45–0.82) with aTNF+LEF and by 0.86 (99% CI: 0.60–1.12) with anti-TNF+other DMARDs during the first year after treatment initiation. Depending on the absolute level of disease activity, DAS28 improvements between 0.6 and 1.2 are considered moderate therapeutic responses and improvements greater than 1.2 are considered good therapeutic responses (European League Against Rheumatism (EULAR) response criteria).29 Overall, 62% of all patients receiving anti-TNF agents in combination with conventional DMARDs were considered responders after 1 year, 19% as having a good response and 44.5% as having moderate response. The proportion of good and moderate responders did not differ significantly between the three groups (p = 0.06) after correcting for differences in baseline covariates. Significant predictors greater improvements in disease activity after treatment initiation were younger age (p<0.001), male gender (p<0.006), lower functional disability at baseline as measured by the HAQ (p<0.001), abscence of rheumatoid factor (p = 0.001), no need for concomitant glucocorticoids (p<0.001) and no prior failure on prior anti-TNF agent (p = 0.01).
Tolerability and safety
A total of 178 combination therapies were interrupted because of adverse events (28%). The most common adverse events leading to treatment interruption were allergic reactions (28%), infections (19%), skin reactions (19%), and gastrointestinal side effects (12%). Hepatotoxicity (2%) and malignancies (6%) were rare causes of treatment interruption in this cohort. We found no difference between the three combinations of conventional DMARDs and anti-TNF agents in the overall incidence of side effects (ANOVA, p = 0.13), or in time to the occurrence of side effects (ANOVA, p = 0.24). Furthermore, we did not find significant differences between these combinations in the specific types of adverse events, with the exception of allergic complications that were reported slightly less often with the combination anti-TNF+MTX (HR: 0.45, 98% CI: 0.20–0.98) than with the other two combinations (ANOVA, p = 0.04). In particular, no trend for an increasing incidence of dermatological adverse events was found with the combination anti-TNF+LEF, (ANOVA, p = 0.18), which had been previously described.4 11 However, the total numbers of events for the specific side effects were low.
DISCUSSION
We studied the effectiveness and safety of the combination of anti-TNF+LEF as compared to the combination of anti-TNF+MTX and anti-TNF+other DMARDs in a population-based cohort of 1281 patients with RA. The overall discontinuation rates of these combinations were relatively high with a median survival of only 16 months (IQR: 10–37), but the discontinuation rates did not differ between the three regimens. The retention of the individual anti-TNF agents was significantly longer (median survival of 31.5 months (IQR: 12–68)) suggesting that doctors confronted with inadequate therapeutic responses or side effects attempt first to modify the co-therapy with conventional DMARDs, before eventually changing the anti-TNF agent. The progression of structural joint damage (radiographic erosion score), functional disability (HAQ) and RA disease activity (DAS28) were also similar in the different regimens. In addition, the analysis of side effects did not show any significant differences regarding the frequency and type of adverse events. Overall these results suggest that LEF and other conventional DMARDs can offer an effective and safe alternative to MTX as a co-therapy in combination with anti-TNF agents.
In this cohort, 21% of all patients on anti-TNF combination therapy had LEF as co-therapy, which appears to be higher than published figures from other registries (9–13%).4 30 This is probably explained by habits of local rheumatologists and the relatively long disease durations of patients enrolled in the SCQM, which often have a history of prior treatment failure on MTX.
Most published reports on the combination of anti-TNF agents and LEF are based on retrospective case series4 6–10 and lack a control groups, which does not permit comparisons with other conventional DMARD combinations such as aTNF+MTX. One prospective cohort study assessed INF in combination with conventional DMARDs and confirmed clinical responses and incidence of adverse events were not different in patients treated with LEF as compared to other conventional DMARDs.13 However, groups were relatively small (LEF group: n = 33) limiting the statistical power to reveal small differences. Interestingly, the median drug survival of the INF–LEF combination was also relatively short (9 months) and drug retention rates were also similar between the different conventional DMARD groups. Other studies have reported conflicting results. More patients withdrew on INF in combination with LEF than in combination with MTX due to adverse events and severe infusion reactions.31 Different combinations of ADA with DMARDs were examined in a recent 12-week open-label multicentre prospective study. The effectiveness of ADA and LEF was lower than ADA and MTX, with significantly fewer patients achieving American College of Rheumatism (ACR) or EULAR responses.14 In addition, the rate of serious adverse events and serious infections were also higher among patients treated with LEF as compared to MTX (8.2% vs 4.6% and 1.1% vs 1.9%, respectively).14
In this study, the reason for discontinuing the combination of anti-TNF and conventional DMARDs was an adverse event in approximately a third of all treatment interruptions, the remainder being justified by treatment inefficacy, patient preferences, remission or low disease activity, pregnancies and other non-toxic causes. These findings are in line with other reports,13 but the incidence of adverse events was lower than some older studies.8 11 This apparent discrepancy could be partially explained by the fact that adverse events tend to be reported only if considered clinically important by doctors. The perception of what side effect is clinically relevant might have changed in recent years, as rheumatologist are more used to manage biological therapies. Furthermore, we analysed only the adverse events that led to treatment discontinuation.
This analysis has potential limitations inherent to the analysis of observational data. We had no control over the treatment assignment of MTX versus LEF or other concomitant DMARDs, which could result in selection bias or confounding by indication. Because no rationale exists for favouring one concomitant DMARD over the other in terms of efficacy, substantial confounding by indication between these groups is unlikely. Confounding by indication is more likely for anti-TNF agents prescribed with or without concomitant DMARDs, which is why we restricted our analysis to only patients receiving anti-TNF agents in combination with conventional DMARD therapy. We found no significant differences in disease characteristics and common predictors of disease progression between the three treatment groups. However, as expected, certain treatment characteristics differed between these groups. While we could adjust our analysis for many important disease and treatment characteristics potentially associated with disease progression, we cannot exclude the possibility of residual confounding or confounding by unmeasured factors.
Concomitant DMARD therapy was defined at anti-TNF therapy initiation; all patients started concomitantly on traditional DMARDs were analysed as such, whether they continued treatment or not. In clinical practice, concomitant therapy with traditional DMARDs is a dynamic process that might not be captured completely with this definition. This is, however, a conservative approach, comparable to an “intention to treat” analysis in randomised trials, which tends to underestimate the true treatment effect. Because the discontinuation rates of these combinations were similar, it is unlikely that drug retention substantially biased the comparison of therapeutic effectiveness between the three antirheumatic regimen. The present analysis offered sufficient power to detect small differences in effectiveness or retention rates between MTX and LEF in combination with anti-TNF agents. However, the “other DMARD” group was relatively small (n = 116) and heterogeneous (including cytotoxic and non-cytotoxic agents), limiting the strength of the conclusions regarding this therapeutic group.
Missing data is another concern with observational studies. In particular, only 84% of all patients had radiographic data for the analysis of radiographic damage progression. Baseline disease characteristics of patients without available radiographs were similar to those included in the present analysis suggesting that the inclusion criteria of the study selected a representative sample of the population. Strengths of this analysis include a true population-based cohort due to the fact that the Swiss authorities recommended enrolment of all patients receiving anti-TNF agents, a systematic prospective ascertainment of a wide variety of potential confounders and longitudinal radiographic data.
In this large population-based cohort, we found no difference in drug discontinuation rates or in effectiveness measures between anti-TNF+MTX, anti-TNF+LEF and anti-TNF+other DMARD. Furthermore, the safety data of the combinations of anti-TNF+LEF and anti-TNF+other DMARD are reassuring and show that these combinations are well tolerated. Taken together, these results suggest that LEF and potentially other DMARDs offer an effective and safe alternative to MTX as co-therapy in combination with anti-TNF agents.
Acknowledgments
We thank the SCQM staff for the data management and support and to participating doctors and patients who made this study possible. We wish to thank specifically those rheumatologists who enrolled large numbers of these patients (10 or more, in order of numbers included): Colla F, Winterthur; Suter JB, Bern; Chamot A-M, Morges; Lehmann T, Bern; Martin A, Liestal; Wicht F, Solothurn; Marbet Grierson G, Olten; Tinner H, Weinfelden; Aellen P, Nyon; Elmiger B, Bern; Hafelin F, Schlieren; Muller-Werth B, Sarnen; Wiedersheim P, St Gallen; Buchler I, St Gallen; Gerster, J-C, Lausanne; Rappoport G, Yverdon-les-Bains; Cunningham T, Geneva; Brucker R, Luzern; Kloti R, Brugg; Glenz D, Visp; Pancaldi P, Muralto; Diethelm U, Mannedorf; Sturzenegger J, Kreuzlingen; Zenklusen C, Neuchatel; Buchard P-A, Sion; Altermatt R, St Gallen; Messikommer M, Visp; Fluck A, Zurich; Wuest P, Basel; Sauvain M-J, Fribourg; Frey D, Basel; Pfister S, Bulach; Thiebaud G, Geneva; Eigenmann B, Zurich; Muff L, Affoltern a Albis; Keller F, Uster; Brunner H, Thun; Schwartz GM, Geneva; Buchs N, Geneva; Ziehmann M, Zurich; Gut C, Reinach; Maager R, Aarau; Raccaud O, Lausanne; Saxer M, Basel; Maclachlan D, Heiden; Laubscher A, Bad Ragaz; Reich-Rutz C, Zurich; Schaub, K, Mannedorf; Schlor-Dorr U, Reinach; Widmer M, Wetzikon; Baumgartner E, Porrentruy; Davoine G-A, Geneva; Christen B, Lugano; Kowalski M, Solothurn; Gratzl S, Basel; Bodmer F, Geneve; Hunkeler M, Neuchatel; Gaeumann U, Murten; Caravatti M, Wetzikon; Lamoth M, Schaffhausen; Schonbachler J, Zurich; Seglias J, Burgdorf. We also wish to specially thank the participating rheumatology clinics who registered a large numbers of these cases (20 or more): Universitatsspital (Michel B), Zurich; Inselspital (Villiger PM), Bern; Kantonsspital (Hasler P), Aarau; Centre Hospitalier Universitaire Vaudois (So AK), Lausanne; Kantonsspital (Rüdt R), Winterthur; Bethesda Spital (Schwarz H), Basel; Felix-Platter-Spital (Tyndal A), Basel; Kantonsspital (von Kempis J), St Gallen; Kantonsspital (Klöti M), Luzern; Hopital Cantonal Universitaire de Genève (Gabay C), Geneva; Triemli Stadtspital (Theiler R), Zürich; Hopital de La Chaux-de-Fonds (Van Lindthoudt D), Neuchatel; Thurgauer Klinik St Katharinental (Forster A), Diessenhofen; aarRehab Schinznach-Bad (Mariacher S), Aarau; Schulthess Klinik (Kramers – de Quervain IA), Zürich; Burgerspital (Bernhard J), Solothurn; Hopital Regional (Meier JL), Delemont.
REFERENCES
Footnotes
Competing interests: None declared.
Funding: AF was funded by a research grant from the Geneva University. SD was funded by the SCQM Foundation. CG by the Swiss National Science Foundation (Grant no. 320000-107592). This study was further partially supported by an unrestricted research grant from Sanofi-Aventis. The SCQM Foundation has received grants from the Swiss Health authorities (BAG), the Swiss Academy for Medical Sciences (SAMW), the JL Warnery Foundation, the Swiss Society of polyarthritic patients (SPV) and pharmaceutical companies (Abbott, Essex, Wyeth, Roche, Bristol-Myers Squibb, Mepha, Novartis, Sanofi-Aventis).