Article Text

Abstract
OBJECTIVE Antiperinuclear factor (APF), “antikeratin antibodies” (“AKA”), and antibodies to human epidermis filaggrin (AFA), are highly specific serological markers of rheumatoid arthritis (RA), which recognise epitopes on various isoforms of (pro)filaggrin. It was proposed that these antibodies are globally named antifilaggrin autoantibodies. Here the diagnostic value of the detection of each one is compared and the overlap between the three tests evaluated.
METHODS 492 serum samples were tested, including 279 RA serum samples, taken from patients in France and Belgium. APF and “AKA” titres were estimated by indirect immunofluorescence, and AFA titres by immunoblotting on filaggrin enriched human epidermis extracts.
RESULTS By a convenient choice of the positivity thresholds, the diagnostic sensitivity and specificity of the tests were shown to be similar (0.52 and 0.97, respectively). Although the antibody titres were strongly correlated, the associations APF-AFA or AFA-“AKA” permitted more than 52% or 55% of RA to be diagnosed, with a specificity of 0.99.
CONCLUSION APF, “AKA”, and AFA detection have a similar diagnostic value. However, because the three tests do not totally overlap, associating APF with “AKA” or AFA with “AKA” can improve diagnostic sensitivity. None of the three antigens used bear all the epitopes recognised by anti-filaggrin autoantibodies.
- rheumatoid arthritis
- antifilaggrin autoantibodies
- antiperinuclear factor
- antikeratin antibodies
Statistics from Altmetric.com
The most commonly used serological criteria for the diagnosis of rheumatoid arthritis (RA), besides rheumatoid factor (RF), were until recently the antiperinuclear factor (APF) and the so called “antikeratin antibodies” (“AKA”) described by Nienhuiset al in 19641 and by Younget al in 1979, respectively.2The diagnostic value of these antibodies was largely confirmed by numerous research groups3-17 and their detection, although mainly restricted to specialised laboratories, is now consensually considered as a valuable tool for the diagnosis of RA. Moreover, they appear precociously and can even precede the clinical onset of the disease.18-21 APF are autoantibodies that recognise antigen(s) on perinuclear granules in superficial cells from human buccal mucosa squamous epithelium.22-27 They are detected by indirect immunofluorescence (IIF) on smears of these cells from healthy donors. “AKA” are antibodies that decorate the stratum corneum of the rat oesophagus epithelium when detected by IIF on cryosections.2 ,15 ,27-29 We demonstrated that the latter are IgG15 ,30 autoantibodies31 ,32 that do not recognise cytokeratins33-35 but epitopes on a neutral/acidic variant of human epidermis filaggrin,32 a terminal differentiation protein involved in the aggregation of cytokeratin filaments during cornification.36-38 For 16 years, APF and “AKA” were thought to be independent antibody families despite numerous common features.17 ,39 Recently, we reported the identification of the antigen recognised by APF on human buccal mucosa cells39 and showed, using short series of typical RA serum samples, that APF and “AKA” correspond to largely overlapping antibody populations that recognise epitopes borne by human epidermis filaggrin and by closely related proteins from human buccal mucosa cells or from the stratum corneum of the rat oesophagus epithelium.40 We proposed the name “antifilaggrin autoantibodies” to include the two antibody populations.
We subsequently developed diagnostic tests by immunoblotting, using either an extract enriched with the rat oesophagus antigens,41 or a filaggrin enriched epidermis extract.42 The detection of antibodies to human epidermis filaggrin (AFA), validated on a large series of 670 serum samples from patients with RA and other rheumatic diseases, showed diagnostic performances similar to those of “AKA” detection (almost 40% of RA were diagnosed with a specificity of 0.99). However, the results of “AKA” and AFA detection were found to be not totally superimposable. This allowed us to propose a diagnostic test associating “AKA” and AFA detection. Choosing convenient titre thresholds, such a test was able to diagnose 60% of RA, keeping a specificity of 0.99.
Although APF, “AKA”, and AFA are largely the same antifilaggrin autoantibodies (the abbreviations being maintained throughout the paper in reference to the different methods used for their detection), some arguments seemed to indicate that they did not totally overlap. Indeed, the immunofluorescence intensity produced by RA serum on rat oesophagus was largely, but only partially, decreased by immunoadsorption on the neutral-acidic variant of filaggrin.32 Similarly, the absorption of the APF reactivities on the same antigen was found to be incomplete with some RA serum samples.39 Therefore, the questions remaining to be answered were: Are the diagnostic value of the three detection methods identical? Are all the APF positive serum samples “AKA” and/or AFA positive? If not, does the association of APF with “AKA” and/or AFA detection present higher diagnostic performance than each test considered separately? Finally, is APF antigen immunologically closer to human epidermis filaggrin recognised by AFA than to the rat oesophagus antigen recognised by “AKA”?
This work thus constitutes the first study to report the comparative analysis of APF, “AKA”, and AFA detection on a large series of patients.
Methods
SERUM SAMPLES
A total of 492 serum samples (table 1) were obtained from 279 patients with RA classified according to the criteria of the American Rheumatism Association43 and from 213 patients with non-RA arthritides (control serum samples). Patients with non-inflammatory rheumatic diseases were excluded from the study. The patients came from the departments of rheumatology of the Purpan and Rangueil hospitals, Toulouse, France (210 RA and 155 controls), and from the department of rheumatology of Gent hospital, Belgium (69 RA and 58 controls). The serum samples were aliquoted and stored at −80°C until assayed.
Details of patients
APF DETECTION AND TITRATION BY INDIRECT IMMUNOFLUORESCENCE
Briefly, fresh buccal mucosa cells were obtained by scraping the inner cheek of a previously identified good donor. The cells were brought into suspension in phosphate buffered saline (PBS) then collected by centrifugation. The buccal mucosa cells were then resuspended in PBS (100 000 cells per ml), spotted on a microscopic multi-hole slide, and air dried. Serum samples, diluted to 1:5 in PBS, were incubated for 90 minutes at room temperature. Fluorescein isothiocyanate labelled (FITC) goat immunoglobulin Fab fragments to human IgG (γ) (Biosys, Compiègne, France) diluted to 5 μg/ml in PBS were incubated for 30 minutes at room temperature. The preparations were counterstained with ethidiumbromide (100 μg/ml) and mounted.
A serum sample was considered positive if the typical perinuclear staining was seen in at least a few cells. One serum with strong APF reactivity was chosen as the standard serum. An end point titration series of this serum was analysed in parallel with each APF test. Positive serum samples were further diluted until the fluorescence staining disappeared (end point titration). The titres were subsequently transformed into a U/ml format.44
“AKA” DETECTION AND TITRATION BY INDIRECT IMMUNOFLUORESCENCE
A previously described15 semiquantitative IIF assay, was used for the detection and titration of “AKA” on rat oesophagus cryosections.
Briefly, cryostat sections from the middle third of rat oesophagus epithelium, fixed by air drying and rehydrated in PBS, were incubated with human serum diluted to 1:10 in PBS for 30 minutes at 37°C, then incubated for 30 minutes at 37°C with the same secondary antibody as above diluted to 20 μg/ml in PBS. The fluorescence intensity of the stratum corneum of the rat oesophagus epithelium was evaluated on an arbitrary semiquantitative scale from 0 to 4 (0.25 unit steps) by two readers uninformed of the clinical context. The results were summed to obtain a titre-like value ranging from 0 to 8 (referred to as titre throughout the paper). All the serum samples were tested in duplicate within different series.
AFA DETECTION AND TITRATION BY IMMUNOBLOTTING
AFA were detected and titrated by immunoblotting on human epidermis protein extracts enriched with the neutral-acidic variant of filaggrin following the method previously published.32 ,42
Briefly, filaggrin enriched protein extracts from normal human breast epidermis were separated by SDS-PAGE and electrotransferred onto nitrocellulose membranes. The membranes were “blocked” for 30 minutes at room temperature with TRIS-HCl, 150 mM NaCl, pH 8, containing 0.05% Tween-20 (working buffer), then incubated for 60 minutes at 20°C with serum samples diluted to 1:30 in TRIS-HCl, 2 M NaCl, pH 8, 0.05% Tween-20. The membranes were treated for 60 minutes at 20°C with peroxidase conjugated goat antibodies to human IgG(γ) (Southern Biotech, Birmingham, AL) diluted to 1:400 in working buffer. The colour reaction was developed by incubation with 0.5 mg/ml 4-chloro-1-naphthol (Bio-Rad), 0.025% (v/v) hydrogen peroxide, 17% methanol (v/v).
As for IIF, the intensity of labelling (referred to as titre) was estimated according to a semiquantitative scale by two readers uninformed of the clinical context. A pool of highly positive RA serum samples was tested with each membrane and used as reference to correct interassay variations. All the samples were tested at least in duplicate on different membranes.
RF DETECTION AND TITRATION
RF were detected by the classic Waaler-Rose and Latex fixation methods.
DATA ANALYSES
Data analyses were performed using STATISTICA for Windows (StatSoft, Tulsa, OK). Median differences were tested with the Mann-Whitney U test, correlations were sought by computing Spearman’s rank correlation coefficient and the χ2 test was used to compare percentages. The diagnostic value of the various tests was assessed by computing diagnostic sensitivity and specificity and the 0.05 confidence interval.
Results
The results of the three tests did not show any differences in distribution shape, median or range between the 365 serum samples from France and the 127 serum samples from Belgium. The series were consequently combined for the following analyses.
TITRE DISTRIBUTION OF APF, “AKA”, AND AFA
For the three tests, the antibody titres ranged all along the scale (fig 1). However, in the large majority of control samples, the specific antibodies were either undetectable (APF, AFA) or present with a low titre (“AKA”).

Titre distribution of APF, “AKA”, and AFA in RA and control serum samples. APF titre is given as U/ml. “AKA” and AFA titres correspond to a semiquantitative evaluation of the immunoreactivity by indirect immunofluorescence on rat oesophagus cryosections and by immunoblotting on filaggrin enriched human epidermis extract, respectively. Black bars: RA samples; empty bars: control samples. The number of samples is indicated for the bars off the scale.
For the detection of APF, the titre ranged from 0 to 200 U/ml (median = 1.6 U/ml) in the RA samples and from 0 to 100 U/ml (median = 0) in the control samples. Diagnostic specificities of 0.934 and of 0.986 were obtained with titre thresholds of 0.2 U/ml and 6.3 U/ml, respectively. These thresholds were chosen for the further comparisons of the diagnostic sensitivities of the three tests (table 2).
Diagnostic indices
For the detection of “AKA”, the titre ranged from 0.00 to 7.25 (median = 1.50) in the RA samples and from 0 to 2.00 (median = 0.50) in the control samples. In agreement with our previous work,15 ,35 ,42 from and above a titre of 1.50 or 2.00, only a few control samples (seven or one, respectively) were detected, permitting, a diagnostic specificity of 0.967 or 0.995 to be reached, respectively.
For the detection of AFA, the titre ranged from 0.00 to 8.00 (median = 1.00) in the RA samples and from 0 to 7.25 (median = 0.00) in the control samples. The 0.25 threshold, the first step of the semiquantitative scale, allowed RA to be diagnosed with a specificity of 0.934 and the 2.25 threshold allowed a diagnostic specificity of 0.986 to be reached.
DIAGNOSTIC INDICES
The ROC curves (fig 2) show that the three tests presented roughly similar diagnostic performances. Moreover, the three curves approximately intersect at a single point: sensitivity = 0.520, specificity = 0.965. However, for a specificity of 0.950, the diagnostic sensitivity of APF detection was higher than that of “AKA” and AFA detection. Conversely, for a diagnostic specificity higher than 0.980, the sensitivity of “AKA” detection was higher than that of AFA and mostly APF detection (table 2).

Receiver operating characteristic (ROC) curves of APF, “AKA”, and AFA detection. For the three tests, the diagnostic sensitivity (rate of true positives) is plotted compared with 1-specificity (rate of false positive). The portion of curves corresponding to the lowest rate of false positives shows differences between the diagnostic sensitivities of the tests when the specificity ranges from 0.95 to 1.00.
At the 0.95 specificity thresholds, 27 control samples were found to be positive with at least one test. Among them, 16 samples were from patients with systemic autoimmune diseases and 11 from patients with other arthritides. The proportions of false positives within these two groups of control samples were not significantly different.
CORRELATIONS
The titres of APF, “AKA”, and AFA were found to be independent of age, while a higher proportion of positive samples was found in RA serum samples from men than from women (roughly 70% versus 50% at the 95% positivity threshold). A similar relation was found between sex and RF detection.
The titres of APF, “AKA”, and AFA were found to be significantly correlated with RF titres whatever its detection method. However, a noticeable proportion of RF negative RA samples were positive for APF and/or “AKA” and/or AFA (46%, 31%, and 42% at the 0.95 specificity threshold, respectively).
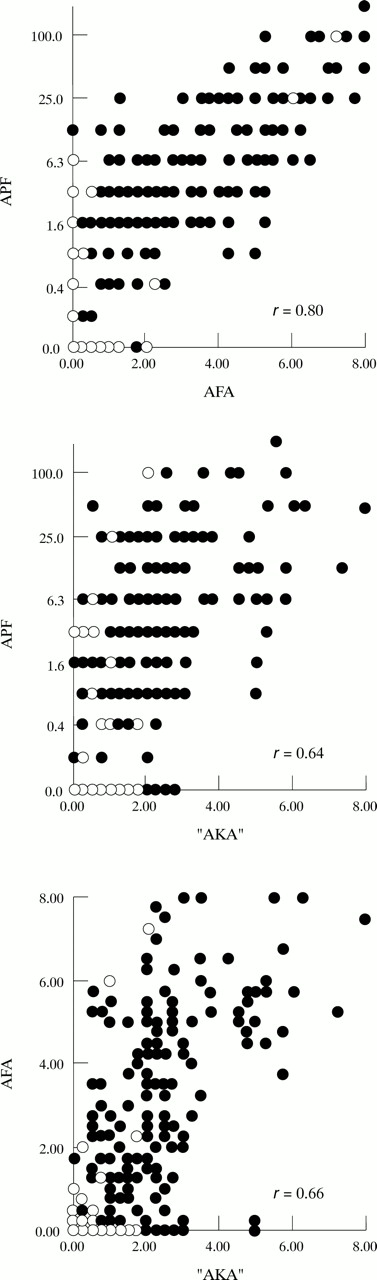
The titres obtained with the three tests were significantly correlated to each other (fig 3). Moreover, the correlation was found to be stronger between APF and AFA than between APF and “AKA” or AFA and “AKA” (p<0.001).

{kind=link}
{kind=link}
{kind=link}
Correlation between the titres of APF, “AKA”, and AFA in RA and control serum samples. The correlation coefficients (r) were computed only for RA samples. The three correlation coefficients are highly significant (p<10-6). Black dots: RA samples; empty dots: control samples.
Despite these significant correlations, some samples were discordant—that is, positive with one or two detection method(s) and negative with the other(s) (table 3). Among the 208 RA samples positive with at least one test, 119 (57%) were concordant for the three tests and 171 (82.2%), for at least two tests. Conversely, among the 27 control samples positive with at least one test, only two (7.4%) were concordant for the three tests and six (22.2%) for at least two tests.
Distribution of RA and control serum samples with regard to “AKA”, AFA, and APF positivity
Consequently, an association of two or three tests, which would permit a higher diagnostic sensitivity to be obtained without loss of specificity, was sought by analysing the diagnostic indices at various combinations of the positivity thresholds. For a diagnostic specificity of 0.99, the more efficient associations were (AFA>0 and “AKA”>0.5) and (APF>0.6 and “AKA”>0.5), which allowed 55% and 52% of RA to be diagnosed, respectively.
Discussion
To assess the diagnostic value of APF compared with “AKA” and AFA detection in actual conditions of use—that is, when the tests are ordered for patients with arthritides—we chose control serum samples only from patients with non-RA inflammatory rheumatic diseases. In these conditions, the distribution of “AKA” and AFA titres in RA and control samples was found to be similar to that we previously reported,42 confirming that the rate of false positives is not higher among samples from patients with arthritides than among samples from patients with non-inflammatory rheumatic diseases.15 ,42 The distribution of APF titres showed striking similarities with the distribution of AFA titres. Particularly, in the majority of control samples, antibodies were undetectable, allowing, for the lowest titre, a good specificity (0.93) to be obtained with both tests. At this specificity threshold, APF detection presented a higher diagnostic sensitivity (0.67) than AFA (0.57) or “AKA” detection (0.57, computed by interpolation from the ROC curves). Conversely, for a specificity near 0.99, APF detection allowed less than 30% of RA to be diagnosed compared with 40% with “AKA” and 37% with AFA detection. Despite the differences, the three tests can be considered to have similar diagnostic sensitivity and specificity. A survey of the diagnostic indices reported in the medical literature17 shows that the values we report in this study, largely agree with those previously obtained in comparable technical conditions. Indeed, we reported15 that on the whole data from the published series on IgG “AKA” detection, the sensitivity was 0.46 and the specificity, 0.97. For APF detection, a similar computation shows that the sensitivity of the test was 0.72 when the specificity was 0.92.45 These indices could be plotted close to the ROC curves shown in figure 2 and thus do not differ from those reported in this study.
Although APF, “AKA”, and AFA titres were strongly correlated with each other, we found some serum samples (mainly control samples) positive with one or two tests and negative with the other(s), whatever the chosen positivity threshold. We thus explored whether a combination of two or three tests, with convenient positivity thresholds, would allow sensitivity to be increased, keeping a high diagnostic specificity (⩾0.99). No combinations of the three tests were found to be sufficiently convincing to be proposed as a valuable diagnostic test for RA. Whereas the association APF/“AKA” allowed a sensitivity of 0.52 to be reached, the association of “AKA” with AFA detection remained the most efficient, with a sensitivity of 0.55 in the present series of patients compared with 0.60 in a previous study using a partially overlapping (263 of 492) series.42Recently,46 an enzyme linked immunosorbent assay (ELISA), using high performance liquid chromatography purified filaggrin, was developed. Prevalidated on short series of serum samples, the test showed diagnostic indices close to those of APF, “AKA”, and AFA detection. Comparatively validated on large series of patients, such a test could be a valuable alternative to AFA detection by immunoblotting.
Despite the correlations between APF, “AKA”, and AFA titres, it was obvious, considering the whole series, that the three antibody populations do not totally overlap. Indeed, for example, we found 19 RA serum samples with significant APF titres and undetectable AFA and “AKA”. We previously reported similar discrepancies between “AKA” and AFA detection42 and hypothesised that this could be explained by differences in antigen conformation between the two immunodetection methods and in biochemical properties of the recognised antigens. In this study, however, we found a significantly higher correlation between APF and AFA than between APF and “AKA”, although in the latter case, a similar IIF method was used to detect the antibodies. Consequently, it can be assumed that the differences of immunoreactivity mainly result from differences in the nature of the antigens, as it is highly probable that human epidermis filaggrin and the APF defined profilaggrin isoforms share more numerous epitopes39 than these human proteins and the rat oesophagus antigen defined by “AKA” do. However, none of the three antigens bear all the epitopes potentially recognisable by RA serum samples. The population of antifilaggrin autoantibodies constituted by the three overlapping APF, “AKA”, and AFA antibody families, thus recognises a spectrum of epitopes, probably all presented by the eliciting antigen, but only partially shared by the three antigens used for APF, “AKA”, and AFA detection.
Recently, we have demonstrated47 together with others48 that the epitopes on human filaggrin are generated by a post-translational modification, namely by the transformation of arginine residues into citrulline by a peptidylarginine deiminase. Moreover, we showed49 that (pro)filaggrin related antigens from human buccal mucosa and rat oesophagus epithelium are also deiminated. Additionally, antibodies from RA serum samples, affinity purified on a citrulline containing peptide from filaggrin were shown to be positive with the APF and “AKA” tests.48 The identification of immunoreactive citrullin containing peptides48 50 will allow new immunoassays to be developed. A multi-ELISA48 has already shown a high diagnostic value (sensitivity 76%, specificity 96%). Whether such a test will allow all the RA patients who are positive with APF, “AKA” or AFA tests to be diagnosed remains to be demonstrated.
To conclude, we showed in this study that APF detection and titration, using a secondary antibody specific for human IgG, present similar diagnostic performances to that of “AKA” or AFA detection. Because the three tests do not totally overlap, we also showed that the association of APF and “AKA” or AFA and “AKA” can significantly improve the diagnostic sensitivity, without loss of specificity. Lastly, as none of the three antigens used bear all the epitopes recognised by RA serum samples, the eliciting antigen remains to be identified. We are now attempting to localise such an antigen in the rheumatoid articular tissues that shares epitopes with the various isoforms of (pro)filaggrin specifically recognised by RA serum samples.
Acknowledgments
We thank Professor M Costagliola (Plastic Surgery Department, Rangueil Hospital, Toulouse) for providing human skin, Professor B Fournié, A Cantagrel and B Mazières (Rheumatology Departments, Purpan and Rangueil Hospitals, Toulouse) for providing human serum samples and clinical data. We also thank M-F Isaia, M-P Cazevieille and A Heirwegh for their valuable technical assistance.
References
Footnotes
Funding: this work was supported by grants from the “Association pour la Recherche sur la Polyarthrite”, the “Université Paul Sabatier”, Toulouse (JE-DGRT 1965), the “Institut National de la Santé et de la Recherche Médicale” (CJF 96–02), the “Région Midi-Pyrénées” and the NFWO (grant 3.0028.95).