Article Text

Abstract
OBJECTIVE To determine the current prevalence of hyperuricaemia and gout in New Zealand Maori and Europeans for comparison with previous studies.
METHODS 342 Maori and 315 European men and women aged 15 years and older were studied by personal interview and a musculoskeletal system examination. The 1977 ARA criteria for gout in a survey setting were used and serum uric acid was determined by a uricase method. The data were compared with those of previous New Zealand studies.
RESULTS Gout was significantly more common in Maori (6.4%) than Europeans (2.9%) (Δ = 3.6%, 95% confidence interval 0.4 to 6.8) and in Maori men (13.9%) than in European men (5.8%) (Δ = 8.1%, 95% CI 1.0 to 15.2). Hyperuricaemia was significantly more common in Maori men (27.1%) than in European men (9.4%) (Δ = 17.7%, 95% CI 8.3 to 27.1) and in Maori women (26.6%) than in European women (10.5%) (Δ = 16.1%, 95% CI 8.5 to 23.7). At least 14% of hyperuricaemic individuals were receiving diuretics, of whom 78% were women. Comparison with previous studies shows that the prevalence of gout has increased in both Maori and Europeans, particularly in men. In Maori men the prevalence of gout has risen from 4.5–10.4% previously to 13.9%, and in European men from 0.7%–2.0% previously to 5.8%. Clinical differences included a stronger family history, earlier age at onset, and a higher frequency of tophi and polyarticular gout in Maori than Europeans. Of those with gout, 62% of Maori and 63% of Europeans were hyperuricaemic on the day surveyed and six (19.4%) were on diuretics. Treatment of gout was inadequate in most cases.
CONCLUSIONS Hyperuricaemia and gout remain common among Maori. Of concern is that the prevalence of gout appears to be on the increase, not only in Maori but also in Europeans in New Zealand.
- hyperuricaemia
- gout
- Maori
Statistics from Altmetric.com
Gout is the commonest form of inflammatory arthritis in men over the age of 40 and appears to be on the increase.1 In the USA the self reported prevalence of gout almost trebled in men aged 45 to 64 years between 1969 and 19812 and in Finland there was a 10-fold increase in gout or hyperuricaemia over an eight year period.3 Reasons for the rising prevalence of gout include dietary changes, environmental factors, increasing longevity, subclinical renal impairment, and the increased use of drugs causing hyperuricaemia, particularly diuretics.1-5
Maori are prone to hyperuricaemia6–11 and gout is common, ranging from 4.5% to 10.4% in men and up to 2.0% in women.6-12 In the two studies performed in New Zealand Europeans the prevalence of gout in men was 0.7%12 and 2.0%,8 ,9 with no cases documented in women.
There have been no epidemiological studies in Maori since 197810 and the studies in Europeans date back to 195812 and 1966.8 ,9 In view of the increasing prevalence of gout elsewhere1–5 we thought it timely to determine the current prevalence of hyperuricaemia and gout in Maori and Europeans to document whether any changes have occurred in New Zealand.
Methods
An epidemiological survey of rheumatic disease was conducted in Rotorua, a city of 65 000 people, predominantly of Maori and European origin, situated 240 km south east of Auckland in the centre of a geothermal region of the North Island, and in Ruatahuna, an isolated village inhabited mainly by Maori of the Tuhoe (“Children of the Mist”) tribe in the heart of the Urewera area, 165 km from Rotorua.
Maori and European subjects aged 15 years and older living in Rotorua were randomly selected from schools and from the Rotorua District Council electoral roll of 1992 and the Eastern Maori District habitation index of June 1990. Random selection of Maori of the Arawa (Rotorua) and Tuhoe (Ruatahuna) tribes was not possible. Traditional beliefs favoured participation by all, as opposed to random selection. Two senior members of each tribe were therefore elected by the elders to recruit as many members as possible to participate, irrespective of whether or not they had a musculoskeletal system complaint. This paper reports data for gout and hyperuricaemia for subjects aged 15 years and older.
After obtaining informed consent from each subject, parent, or guardian, the following information was obtained by personal interview: (1) demographic: name, age, gender, ethnicity; (2) a general medical and a detailed rheumatological history and current/past medications. Answers were entered as “yes”, “no”, or “don’t know”. If an answer was declined the question was left blank. An examination of the musculoskeletal system was then performed. Subjects were classified Maori if they claimed 25% or more Maori ancestry. Six individuals who were neither Maori nor European were excluded from the analysis. Serum uric acid (SUA) levels were determined by a standard uricase method.13 The reference range was 0.15-0.40 mmol litre-1. Hyperuricaemia was defined as >0.42 mmol litre-1 in men and >0.36 mmol litre-1 in women.
Gout was diagnosed if six or more of the 11 American Rheumatism Association (ARA) criteria for gout in a survey setting were present.14 All individuals who had ever had gout were included, irrespective of when the last acute episode occurred.X rays were performed and general practitioner, hospital, and other records were examined where available to validate the diagnosis. Additional information obtained from those with gout included: family history, age at onset of gout, the clinical picture, and natural history.
The criteria for gout used in previous studies were applied to our subjects for comparison. These were: (1) severe, episodic, acute, peripheral, asymmetric arthritis with complete resolution and hyperuricaemia12; (2) two of three of the following: (a) typical acute arthritis, usually podagra lasting two weeks, followed by complete resolution, (b) good response to colchicine, (c) hyperuricaemia6 8 9; (3) two or more typical attacks of podagra affecting the great toe. Hyperuricaemia was not used as a criterion.10 The criteria used by Gibson et al 11 were not specified.
The data for mean serum uric acid concentrations, hyperuricaemia, and gout were analysed as follows:
- (1)
- Maori/European comparison;
- (2)
- Urban (Arawa)/rural (Tuhoe) comparison;
- (3)
- the findings in the present study were compared with previous studies to determine whether any changes had occurred. The comparison took into account differences in survey methods, criteria for gout, whether individuals who had ever had an attack of gout or only those whose last acute episode had occurred within the previous 12 months were included, the definition of hyperuricaemia, and the assay method used. For comparison with previous studies a factor of 0.0598 was used to convert mg 100 ml-1 to mmol litre-1where necessary and two suggested quantities, 0.06 mmol litre-1 and 0.034 mmol litre-1,15,16 were added to our serum uric acid concentrations to adjust for the higher values obtained by non-enzymatic methods.
On completion of the survey, meetings were held to convey the findings to the participants.
STATISTICAL ANALYSIS
Data were analysed using the Statistical package for social sciences release 4.1 on the University of Otago VAX/VMS system. To compare the prevalence of gout between Maori and Europeans, and between Maori men and European men, Mantel-Haenszel age adjusted relative risks were calculated. Analysis of variance was used to test for differences in uric acid concentrations between ethnic and gender groups, with age as a covariate. After adding 0.06 or 0.034 mmol litre-1 to serum uric acid concentrations, Student’st test was used to test for differences within each age group between uric acid concentrations from this study and those of previously reported studies. A P value of less than 0.05 was considered to be statistically significant.
Results
DEMOGRAPHY
Of the 657 Maori and European subjects aged 15 years and older, 342 (52.1%) were Maori, mean age 40.5 (SD 16.5) years, and 315 (47.9%) were Europeans, mean age 50.5 (16.1) years. The Maori sample was significantly younger than the European group (Δ = 10 years, 95% confidence interval 7.5 to 12.5). The sex distribution was similar for Maori (62.3% women, 37.7% men) and Europeans (55.6% women, 44.4% men).
Of 289 Rotorua subjects asked whether they were living in Rotorua specifically because of a musculoskeletal system disorder only two (0.7%) said they were.
PREVALENCE OF GOUT
The cumulative prevalence of gout in the 657 subjects aged 15 years and older was 31 (4.7%). Significantly more were Maori (22/342, 6.4%) than Europeans (9/315, 2.9%) (age adjusted relative risk = 3.2, 95% confidence interval 1.6 to 6.6) and the prevalence was higher in Maori men (18/130, 13.9%) than in European men (8/139, 5.8%) (age adjusted relative risk = 4.0, 95% confidence interval 1.8 to 8.5). The sex ratio of Maori men to women with gout was 5:1 and of European men to women, 8:1. If only those whose last acute attack had occurred within the preceding 12 months were included, the prevalence of gout would have been 25% lower than reported here.
There were no urban/rural differences in the prevalence of gout in Maori men. All four Maori women with gout were from Rotorua which may be coincidental.
SERUM URIC ACID
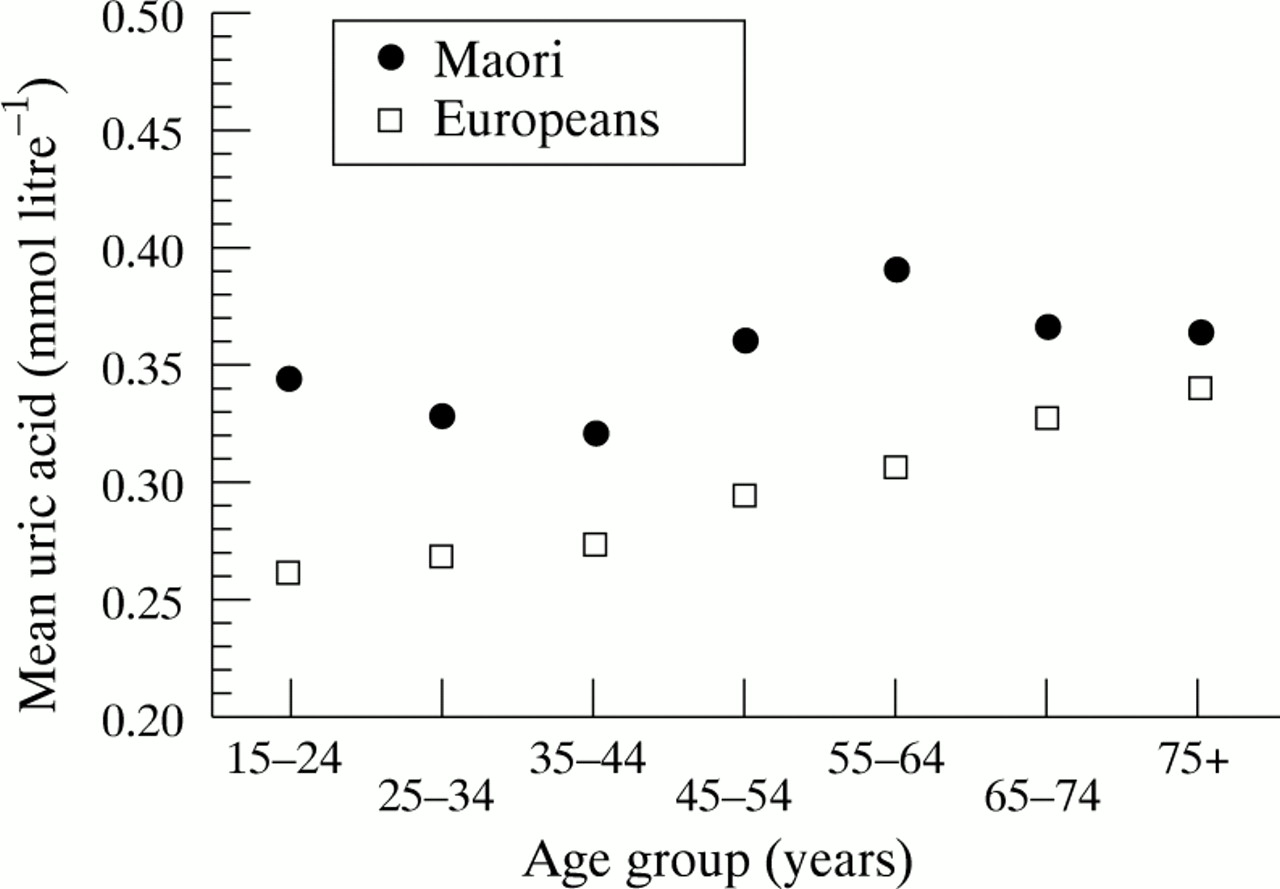
Age adjusted mean serum uric acid was higher for Maori than for Europeans (0.35 and 0.29 mmol litre-1 respectively, P = 0.001). Mean serum uric acid showed an increase with age and values were higher in Maori than in Europeans (figure). Two factor analysis of variance controlling for age showed that mean serum uric acid concentrations were significantly higher in Maori men than in Maori women, in European men than in European women (F = 128.8, df = 1, P = 0.001), in Maori men than in European men, and in Maori women than in European women (F = 129.6, df = 1, P = 0.001).

{kind=link}
Mean serum uric acid concentrations in Maori and Europeans by age group.
Hyperuricaemia was significantly more common in Maori men (27.1%) than in European men (9.4%) (Δ = 17.7%, 95% confidence interval 8.3 to 27.1) and in Maori women (26.6%) than in European women (10.5%) (Δ = 16.1%, 95% confidence interval 8.5 to 23.7). Sixty two per cent of Maori and 63% of Europeans with gout were hyperuricaemic on the day they were surveyed. Marked hyperuricaemia (> 0.54 mmol litre-1) was more common in Maori men (6.8%) than in European men (2.2%) but the difference did not reach significance (Δ = 4.6%, 95% confidence interval −0.5 to 9.8). At least 14% of the hyperuricaemic individuals were receiving diuretics, of whom 78% were women.
There were no urban/rural Maori differences in mean serum uric acid concentrations or hyperuricaemia.
CLINICAL ASPECTS
The mean age at onset of gout in Maori was 46 years (range 21 to 72) and in Europeans 50 years (range 34 to 64). Three Maori men had developed gout by age 28 years. The commonest mode of onset in Maori and Europeans for both men and women was podagra (78%). The course was monarticular or pauciarticular in 60% and polyarticular in 40% of cases. Of those with polyarticular gout 90% were Maori. Tophi were present in one European man and in four Maori men, one of whom was 26 years old with severe widespread tophaceous deposits. In most cases treatment for gout consisted of non-steroidal anti-inflammatory drugs (NSAID) or colchicine. The majority, mainly Maori, had either never taken a hypouricaemic agent, either by choice or by not being offered one, or treatment was intermittent, usually because of poor compliance. No urban/rural differences in clinical manifestations were found. Eleven (35.5%) of the 31 subjects had co-existing ischaemic heart disease, diabetes mellitus, or hypertension, one had chronic renal failure, and one had polycythaemia rubra vera. Six (19.4%)—four Maori men and two European men—were on diuretic treatment. There was a stronger family history of gout in Maori than in Europeans.
COMPARISON WITH PREVIOUS STUDIES
Allowing for methodological differences comparison of our data with previous studies showed the following.
Prevalence of gout
The prevalence of gout in our study for both Maori and Europeans was higher than previously reported, particularly in Maori men, suggesting that gout is on the increase in New Zealand (table). Selection of participants in previous studies was by non-random recruitment of as many members of a tribe as possible and random selection of Maori and Europeans in an urban setting,8-10 ,12 as in our study. In one survey6 the whole tribe and in another11 all Maori men working in a factory were recruited. Only one of our 31 subjects with gout, a Maori woman, did not meet the criteria used by Lennane et al 12 and Rose and Prior,6 ,8 ,9 and two subjects, the same Maori woman and a Maori man did not fulfil the Brauer and Prior10 criteria. Even if both these individuals were excluded for the purposes of comparison, the prevalence of gout in our Maori subjects would only drop to 21/342 (6.1%) instead of 6.4%—Maori men 17/130 (13.1%) instead of 13.9% and Maori women 3/212 (1.4%) instead of 1.9%.
Serum uric acid concentrations
Statistical comparison of mean serum uric acid concentrations and hyperuricaemia was possible in two studies.8-10 When 0.06 mmol litre-1 was added to our serum uric acid values to adjust for comparison with the two studies which used a non-enzymatic method, mean serum uric acid concentrations in some age groups were significantly higher, and a tendency to hyperuricaemia greater, in our subjects. These differences were not observed when 0.034 mmol litre-1 was added.
Discussion
The study confirms the high prevalence of gout among Maori. It also shows that the prevalence has increased in both Maori and Europeans compared with previous studies (table). We believe that our sample is representative of Maori and Europeans living elsewhere in New Zealand and therefore that the prevalence of gout has increased nationally. The increase is particularly striking in Maori men6–12 and in European men.8 ,9 ,12 The narrowing gap in the male:female ratio of gout from 20:1 formerly to 1.7-6.6:117 18 in the 1960s was also evident in our study, both in Maori and Europeans.
Confounding factors were considered as a possible source of bias in the comparison of our prevalence figures with those of previous studies. None was thought to influence the comparison significantly. Selection of participants by random and non-random recruitment in the age group 15 years and over in our survey was very similar to those in all the previous studies6 8–10 12 except for one, which was not a population survey and age was not stated.11 We investigated whether the age distribution of our sample differed from that of previous studies, and age adjustment was made where possible. The authors of papers in which comparisons of gout prevalence were made have not reported the age distribution of their gout cases, so neither age stratification nor age standardisation of the data are possible. Furthermore, in each comparison where age distribution of the previous sample was reported, the age distribution was either the same or younger than for our sample. Therefore we are confident that the differences in age structure between our study and those reported earlier did not result in any overestimation of the differences in gout prevalence. Although the ARA criteria used in our survey differed from those of other surveys, we showed that our prevalence figures changed minimally when other criteria were applied to our subjects. The difference was considered too small to influence the comparison. Our study showed that period prevalence of gout was considerably lower than cumulative prevalence. It was therefore important to confirm that prevalence figures in previous studies were also based on cumulative and not period prevalence (Rose BS, Waterworth R, personal communication). Finally the non-random recruitment of subjects, although not ideal, included all members of the tribe and not only those with musculoskeletal system complaints.
Reasons for the increased prevalence of gout in New Zealand are speculative. The eating and drinking habits and diuretic use in our gouty individuals could not be accurately compared with previous studies. However, we suspect that an increase in diuretic use thought to explain the rising prevalence of gout elsewhere2–5 may well be a factor.
Hyperuricaemia19 ,20 and high mean serum uric acid concentrations21 as risk factors for gout have been well documented. We were unable to show whether the increased prevalence of gout was associated with a concomitant increase in mean serum uric acid or hyperuricaemia. Our cut off levels for hyper-uricaemia in men and women were the same as those used in previous studies, thereby eliminating bias. However, the study shows the difficulties and possible sources of error in attempting to compare uricase with non-enzymatic methods for serum uric acid, as the amount added to adjust for the difference in concentrations obtained by the two assays can significantly influence the findings and may be a major source of bias. Adding 0.06 mmol litre-1 to our values suggested that mean serum uric acid and hyperuricaemia had increased over the years. This was not confirmed when 0.034 mmol litre-1 was added. We were therefore not able to show conclusively whether or not serum uric acid concentrations have increased in New Zealand.
The high percentage of Maori with tophaceous and polyarticular gout, the large number of Maori and Europeans with ongoing recurrent acute attacks, and the fact that on the day surveyed 62% of Maori and 63% of Europeans were hyperuricaemic suggest that gout is still inadequately treated. The mainstay of treatment was NSAID or colchicine for acute attacks. Few were receiving hypouricaemic treatment and of those who were, most either used them intermittently or inappropriately for acute attacks. Traditional treatments are still favoured by many Maori, which may account to some extent for the unacceptably high non-compliance rate. There is clearly a need for ongoing education of medical practitioners and patients alike in the management of gout.
Apart from finding that all four Maori women with gout were from Rotorua, no other urban/rural differences in the prevalence of hyperuricaemia or gout or in clinical manifestations were demonstrated. In retrospect this is not surprising given the close proximity of urban and rural areas, the ready access to transport, and the mobility of the Maori population within New Zealand, unlike in countries where there are clear geographical and lifestyle urban/rural differences such as existed in South Africa.22
This study confirms the view of Silman and Hochberg23 that comparison between studies on gout are fraught with difficulties because of methodological differences, such as non-uniformity of criteria for gout or prevalence based on self reported gout (which has been shown to be up to four times higher than the validated occurrence24), differences in the age group studied, which range from 14+ to 40-64 years worldwide,23 and uncertainty whether prevalence figures are based on cumulative, period, or point prevalence, which can profoundly affect prevalence figures.
We used the ARA criteria in preference to the New York criteria25 for the following reasons. (1) One of the four New York criteria is major reduction in objective inflammation with colchicine within 48 hours. NSAID have largely superseded colchicine for treating acute gout and this is therefore of limited value as a criterion nowadays. (2) The ARA criteria are likely to be increasingly used in population surveys, which would facilitate comparison of future surveys with surveys such as ours to determine trends in hyperuricaemia and gout. (3) None of the New Zealand surveys with which we compared ours used the New York criteria, either because they antedated the criteria6 8 9 12 or because of study design.10
Future studies will determine trends in hyperuricaemia and gout. Comparison with other studies would be facilitated and would be more accurate if a standard methodology were used. We suggest that data be obtained by personal interview and physical examination in subjects aged 15 and older, using the ARA criteria to determine the cumulative prevalence of gout, that serum uric acid be assayed by a uricase method, and that hyperuricaemia be defined as > 0.42 mmol litre-1 in men and > 0.36 mmol litre-1 in women.
The higher serum uric acid concentrations in Maori compared with Europeans for all age groups including the 15-19 year group are of interest. We hope to investigate whether this difference exists at birth or whether it develops during early childhood coincident with a change from a milk to a solid diet, as there are dietary differences in the two population groups.
Acknowledgments
The study was funded by the William Barkla Research Fund, Queen Elizabeth Hospital. We thank the nominated members of the Tuhoe and Arawa tribes for recruiting volunteers and for their assistance in obtaining the demographic data.
References
Prevalence of gout in New Zealand