Article Text

Abstract
Objective Allopurinol, an antihyperuricaemic agent, is one of the common causes of life-threatening severe cutaneous adverse reactions (SCAR), including drug rash with eosinophilia and systemic symptoms (DRESS), Stevens–Johnson syndrome (SJS) and toxic epidermal necrosis (TEN). The prognostic factors for allopurinol-related SCAR remain unclear. This study aimed to investigate the relationship of dosing, renal function, plasma levels of oxypurinol and granulysin (a cytotoxic protein of SJS/TEN), the disease severity and mortality in allopurinol-SCAR.
Methods We prospectively enrolled 48 patients with allopurinol-SCAR (26 SJS/TEN and 22 DRESS) and 138 allopurinol-tolerant controls from 2007 to 2012. The human leucocyte antigen (HLA)-B*58:01 status, plasma concentrations of oxypurinol and granulysin were determined.
Results In this cohort, HLA-B*58:01 was strongly associated with allopurinol-SCAR (p<0.001, OR (95% CI) 109 (25 to 481)); however, the initial/maintenance dosages showed no relationship with the disease. Poor renal function was significantly associated with the delayed clearance of plasma oxypurinol, and increased the risk of allopurinol-SCAR (p<0.001, OR (95% CI) 8.0 (3.9 to 17)). Sustained high levels of oxypurinol after allopurinol withdrawal correlated with the poor prognosis of allopurinol-SCAR. In particular, the increased plasma levels of oxypurinol and granulysin linked to the high mortality of allopurinol-SJS/TEN (p<0.01), and strongly associated with prolonged cutaneous reactions in allopurinol-DRESS (p<0.05).
Conclusions Impaired renal function and increased plasma levels of oxypurinol and granulysin correlated with the poor prognosis of allopurinol-SCAR. Allopurinol prescription is suggested to be avoided in subjects with renal insufficiency and HLA-B*58:01 carriers. An early intervention to increase the clearance of plasma oxypurinol may improve the prognosis of allopurinol-SCAR.
- Gout
- Disease Activity
- Treatment
Statistics from Altmetric.com
Introduction
Allopurinol, a xanthine oxidase inhibitor, has been used for decades as the first-line treatment for hyperuricaemia and gout.1–3 Although there are alternatives of allopurinol, such as febuxostat,4 probenecid,5 benzbromarone6 and sulfinpyrazone,7 the convenient, single-dose daily treatment of allopurinol therapy remains the preferred choice of physicians.2 Yet, allopurinol is notorious for inducing hypersensitivity reactions (allopurinol hypersensitivity syndrome), which manifest as a mild skin rash in about 2% of users while about 0.4% develop severe cutaneous adverse reactions (SCAR).8 Allopurinol-SCAR includes drug rash with eosinophilia and systemic symptoms (DRESS), Stevens–Johnson syndrome (SJS) and toxic epidermal necrosis (TEN). Despite rare, SCAR is life-threatening and can result in multiorgan injuries, prolonged hospitalisation and elevated risk of mortality.9
Genetic predisposition has been shown to be an important risk factor for drug hypersensitivity. We previously reported that the human leucocyte antigen (HLA)-B*58:01 allele is strongly associated with allopurinol-SCAR in Han Chinese,10 and this correlation has been validated in different populations.11–14 Yet, HLA-B*58:01 allele is not absolutely necessary and its positive predictive value is estimated to be 2.7% for allopurinol-SCAR, implying that other risk factors are also involved in the pathogenesis.10–14
Oxypurinol, the main metabolite of allopurinol,15 has been considered to possess antigenic properties for the induction of SCAR as it can cause dose-dependent T-cell response in vitro.16 In addition, since oxypurinol is excreted from the body by the kidney, sufficient renal function has been reported to be crucial for allopurinol tolerability, particularly in patients with chronic kidney diseases (CKD).17 We have demonstrated that granulysin, a 15-kDa protein released by activated cytotoxic T cells and natural killer cells, is the critical cytotoxic factor and immune mediator in SJS/TEN.18 ,19 Furthermore, the increased concentration of oxypurinol induced the activation of cytotoxic lymphocytes to release granulysin in the in vitro cultures.16
Despite the importance of allopurinol dosage and the risk of hypersensitivity reactions has been widely accepted since the work of Hande et al,8 ,17 ,20 ,21 there is still uncertainty about the other risk factors. High dosage of allopurinol, especially in the context of impaired renal function, is associated with SCAR.22 Stamp et al23 proposed that an initial dose of 1.5 mg of allopurinol per unit of estimated glomerular filtration rate (eGFR) followed by a slow increase of dose to reach target plasma urate concentrations may reduce the incidence of allopurinol-SCAR. However, the prognostic factors for allopurinol-SCAR remain unclear. This study aimed to analyse the relationship of dosing, plasma concentrations of oxypurinol/granulysin, renal function and the prognosis of allopurinol-SCAR.
Methods
Study population
Patients who fulfilled the consensus diagnostic criteria for SJS/TEN (including SJS, SJS-TEN overlap and TEN) or DRESS,24–27 and had allopurinol as the culprit drug were enrolled at the Chang Gung Memorial Hospital Health System in Taiwan from 2007 to 2012. Briefly, the patients with SJS had widespread macules or blisters and skin detachment of <10% of the body surface area (BSA), the patients with SJS-TEN overlap with blisters or skin detachment of 10% to 29% of BSA and the patients with TEN with widespread blisters and skin detachment >30% of BSA. The criteria and scoring system of DRESS include the following: cutaneous involvement with diffuse maculopapular exanthema, fever, eosinophilia, lymph node enlargement, atypical lymphocytes and internal organ(s) involvement (eg, liver, kidney, central nervous system, lung, heart and muscle) and prolonged time of resolution. Only the probable or definite cases of SJS/TEN or DRESS were enrolled in this study. The Naranjo algorithm28 and the algorithm of drug causality assessment for epidermal necrolysis29 were applied to identify the offending drug as allopurinol. Enrolled patients with SCAR were diagnosed by at least two dermatologists. In addition, we also enrolled 138 allopurinol-tolerant subjects who had received allopurinol for more than 6 months without any adverse reactions from the same hospital. We collected the following information, including age, gender, physical height and weight, alcohol habit, gout, hyperuricaemia, history of drug allergy, diuretics usage, dosage and time period of allopurinol exposure and baseline renal function (ie, the eGFR data obtained at the time or before starting allopurinol). In addition, HLA-B genotypes, plasma concentrations of oxypurinol and granulysin were determined. All of the participants studied were enrolled from Taiwan where 98% of the population is of Han Chinese. The study was approved by the institutional review board. Informed consent was obtained from each participant.
HLA genotyping
The HLA-B genotypes were determined by SeCore HLA Sequence-based typing (Invitrogen, Life Technologies, USA).
Determination of the concentrations of plasma oxypurinol and granulysin, and renal function
The plasma samples were collected from the participants at various time intervals from the last exposure to allopurinol. Blood from allopurinol-tolerant controls was collected at the time points from the last dosage of allopurinol across 12 h intervals when the subjects received the maintenance dosage. The day of allopurinol withdrawal was set as ‘day 0’. The concentrations of plasma oxypurinol in the samples were determined by a validated high-performance liquid chromatography system equipped with an ultraviolet detector employing a wavelength of 254 nm.30 The plasma levels of granulysin were determined by ELISA as described previously.18 Samples were analysed in triplicate. The assay sensitivity for granulysin was 2.5 ng/mL. For renal function, creatinine clearance was determined and the eGFR was calculated using the Modification of Diet in Renal Disease study equation.31
Statistical analysis
Categorical data were compared between groups with use of Fisher's exact tests, and continuous data (presented as mean and SDs or SEM, with range given in parentheses) were compared with use of non-parametric tests. ORs were calculated from the grouped numbers. Weighted linear regression was applied to the oxypurinol and granulysin concentration data with variables of eGFR ≥30 or <30 mL/min/1.73 m2 and mortality of patients with SJS/TEN, as well as the time since last exposure to allopurinol. The statistical analyses, multiple linear regression and multivariate logistic regression analysis were performed with PASW Statistics 18 (formerly SPSS Statistics) (SPSS, Chicago, Illinois, USA). Differences were considered to be statistically significant at p<0.05.
Results
HLA-B*58:01 was strongly associated with allopurinol-SCAR
We enrolled 48 patients with allopurinol-SCAR (26 SJS/TEN and 22 DRESS) and 138 tolerant controls (table 1). The patients with allopurinol-SCAR were slightly older than the tolerant controls (p=0.047). The physical height and weight, alcohol habit, diuretics usage and history of drug (non-steroidal anti-inflammatory drugs or antibiotics) allergy showed no difference between allopurinol-SCAR and tolerant controls (table 1). Women showed 6.94 times higher risk for allopurinol-SCAR (95% CI 3.2 to 15.1, p<0.001) (table 1), which is consistent with the previous studies.32 All of the patients with SCAR and tolerant controls receiving allopurinol were of hyperuricaemia. Gout was found in 66.7% (32/48) of patients with SCAR and in 89.9% (124/138) of tolerant controls (p<0.001) (table 1). Ten (21%) of the 48 patients with SCAR died; all of whom were severe SJS/TEN cases (table 1). HLA-B*58:01 allele showed strong association with allopurinol-SCAR (OR (95% CI) 109 (24.8 to 481), p<0.001) (table 1). There was no significant difference in the initial dosage of allopurinol between the patients with SCAR (mean±SD=138±75.5 mg/day) and tolerant controls (117±43.7 mg/day) (p=0.078) (table 1). The maintenance dosage of allopurinol was significantly higher in the tolerant group (mean±SD=179±66.9 mg/day) than the SCAR group (145±71.4 mg/day) (p=0.005) (table 1). The mean duration of drug exposure in patients with SCAR was 31 days (range 1–86) and in tolerant controls was 25 months (range 6–152) (p<0.001).
Demographic characteristics of allopurinol-tolerant controls and patients with allopurinol-induced severe cutaneous adverse reactions (SCAR)
Impaired renal function increased the risk of allopurinol-SCAR
The baseline eGFR of patients with allopurinol-SCAR was significantly lower than that of tolerant controls (SCAR: 34.0±29.0 vs controls: 67.5±32.4 mL/min/1.73 m2, p<0.001) (table 1). Severe renal impairment (eGFR <30 mL/min/1.73 m2) was detected in 60% (29/48) of cases but only in 15.9% (22/138) of tolerant controls, which showed 8.0 times higher risk for allopurinol-SCAR (95% CI 3.9 to 16.8) (p<0.001) (table 1). The values of initial dosage/eGFR significantly increased in allopurinol-SCAR (8.2±7.6 mg/mL/min) compared with that of tolerant controls (2.7±3.3 mg/mL/min) (p<0.001) (table 1). Of the subjects with renal impairment, there was no significant difference in the values of initial dose/eGFR between allopurinol-SCAR and tolerant controls (table 1). Considering that HLA-B*58:01 is known as a genetic marker for allopurinol-SCAR in Han Chinese, we used the significant factors, including age, gender, presence of comorbidity of gout or renal impairment, found in univariate analysis for a multivariate logistic regression model. Renal impairment was identified as an independent risk factor for allopurinol-SCAR (OR (95% CI) 5.64 (2.46 to 12.9), p<0.001) after the multivariate adjustment (see online supplementary appendix table S1).
Delayed clearance of oxypurinol in patients with SCAR with renal impairment
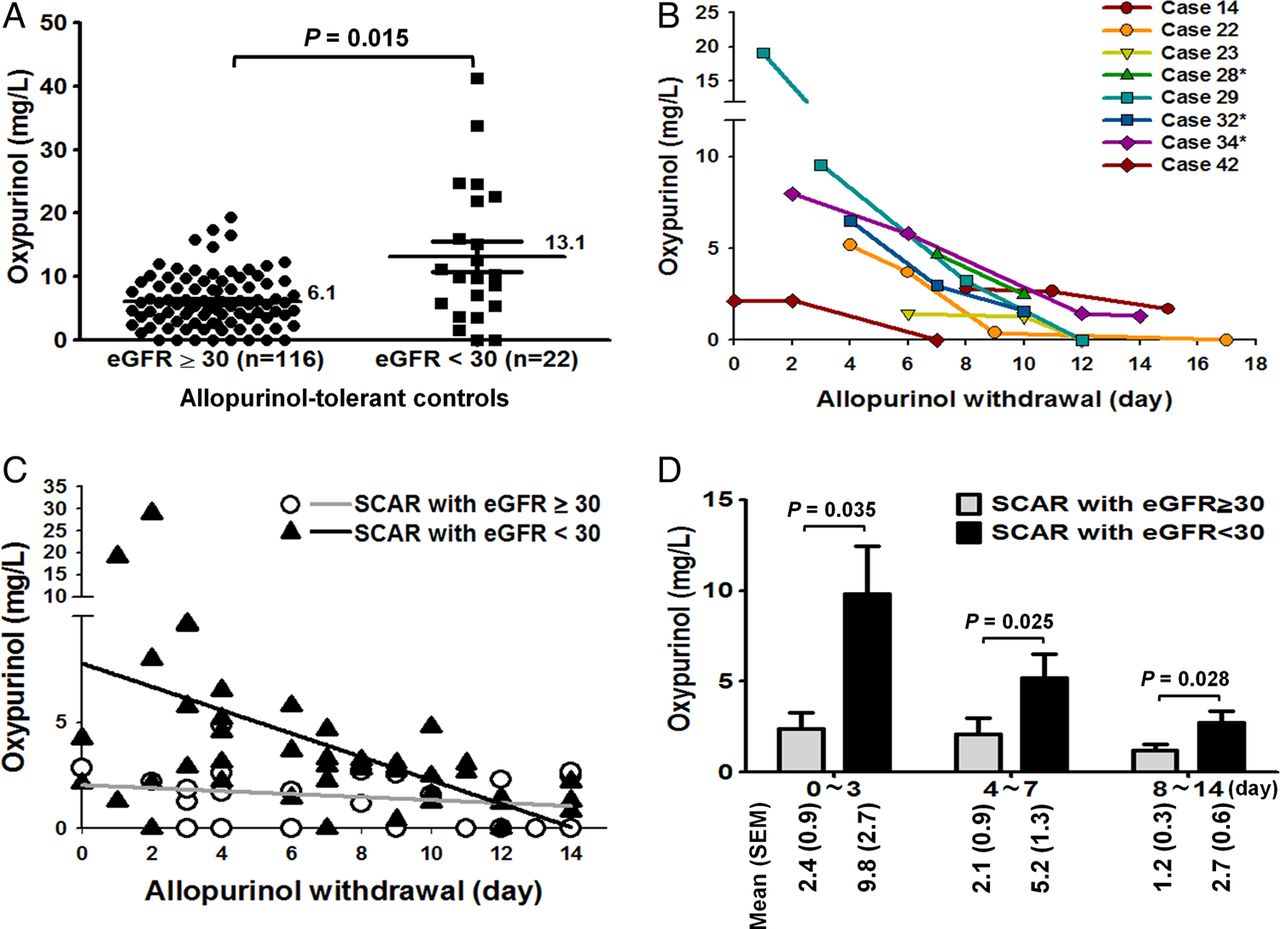
To evaluate the effects of renal function on oxypurinol clearance, we first compared the concentrations of plasma oxypurinol in allopurinol-tolerant controls (figure 1A). Severe renal impairment (eGFR <30) showed higher concentrations of plasma oxypurinol (mean=13.1 mg/L) than those without renal impairment (6.1 mg/L) (p=0.015) (figure 1A). The tolerant subjects with severe renal impairment even had a lower maintenance dosage (mean±SD=148±50.0 mg/day) (table 1). In addition, we found that the diuretics usage did not significantly increase the plasma oxypurinol in the tolerant controls with renal impairment (p=0.077) (see online supplementary appendix figure S1).

Correlation between the concentrations of plasma oxypurinol and renal function in patients with allopurinol- SCAR and tolerant controls. (A) Plasma oxypurinol levels in tolerant controls with or without severe renal impairment (eGFR <30 mL/min/1.73 m2). (B) Serial detection of plasma oxypurinol levels in patients with SCAR with severe renal impairment after allopurinol withdrawal (*deceased cases). (C) Regression equations of oxypurinol levels corresponding to the time after allopurinol withdrawal in patients with allopurinol-SCAR with eGFR <30 mL/min/1.73 m2 or ≥30 mL/min/1.73 m2. (D) The average oxypurinol concentrations at different time intervals after allopurinol withdrawal in patients with allopurinol-SCAR. eGFR, estimated glomerular filtration rate; SCAR, severe cutaneous adverse reactions.
The relationship between renal status and oxypurinol clearance in allopurinol-SCAR was analysed. According to the data of the previous studies, the normal clearance of oxypurinol was defined as plasma oxypurinol concentration ≤1 mg/L after 3 days of allopurinol withdrawal.15 The serial change of plasma oxypurinol of eight patients with SCAR with severe renal impairment is illustrated in figure 1B. Four cases (cases 22, 29, 32 and 34) had remarkably high concentrations of plasma oxypurinol (>5 mg/L) after 4 days of allopurinol withdrawal and three deceased patients (cases 28, 32 and 34) showed extremely slow elimination of plasma oxypurinol (>2 mg/L) after 10 days of allopurinol withdrawal (figure 1B). The regression equation of oxypurinol levels corresponding to the time after allopurinol withdrawal in patients with allopurinol-SCAR with severe renal impairment (y=7.77−0.55x, R=0.44, n=23) was significantly different from that of patients with eGFR ≥30 (y=2.03−0.07x, R=0.23, n=17) (p=0.048) (figure 1C). After allopurinol withdrawal for 0–3 days, the levels of plasma oxypurinol significantly decreased in patients with SCAR with eGFR ≥30 (mean±SEM=2.4±0.9 mg/L) but remained high in the patients with severe renal impairment (9.8±2.7 mg/L) (p=0.035) (figure 1D). Furthermore, after allopurinol withdrawal for 4–7 days or 8–14 days, the levels of plasma oxypurinol were almost undetectable in the patients with SCAR with eGFR ≥30, but still stayed high in patients with SCAR with severe renal impairment (p<0.05) (figure 1D). Delayed clearance of oxypurinol (plasma concentration >1 mg/L after 3 days of allopurinol withdrawal) was detected in 96% of patients with SCAR with severe renal impairment, whereas it was present in only 56% of patients with eGFR ≥30 (p=0.002) (table 2). Using multiple linear regression analysis, plasma oxypurinol concentration would be predicted by the duration of allopurinol withdrawal and eGFR of patients with allopurinol-SCAR with β coefficient of −0.23 (−0.08 to −0.38) and 1.90 (0.19 to 3.60), respectively (see online supplementary appendix table S2). These data revealed delayed clearance of oxypurinol in patients with allopurinol-SCAR with renal impairment.
Delayed clearance of oxypurinol in patients with allopurinol-SCAR*
Renal impairment correlated with poor prognosis of allopurinol-SCAR
Among 26 patients with allopurinol-SJS/TEN, 11 patients with eGFR ≥30 all survived, whereas 10 out of 15 (67%) patients with severe renal impairment proceeded to death, revealing that renal impairment was significantly associated with the mortality of allopurinol-SJS/TEN (p<0.001) (figure 2A). As all of our enrolled patients with allopurinol-DRESS survived, we used ‘the remission duration for cutaneous reactions’ as the index for the prognosis of allopurinol-DRESS. Among 22 patients with allopurinol-DRESS, 8 patients with eGFR ≥30 achieved complete remission of cutaneous reactions within an average of 57.6 days, but the remaining 14 patients with severe renal impairment required longer duration (average 113 days) for completing remission, indicating that renal impairment was associated with the poor prognosis of allopurinol-DRESS (p=0.011) (figure 2B).

Renal function and prognosis of allopurinol-severe cutaneous adverse reactions. (A) The mortality in patients with allopurinol SJS/TEN (n=26) with renal functions of eGFR <30 or ≥30 mL/min/1.73 m2. In ten deceased cases, all had severe renal impairment. (B) Duration for the remission of cutaneous reactions of patients with allopurinol-DRESS (n=22) with different renal function (eGFR <30 or ≥30 mL/min/1.73 m2). eGFR, estimated glomerular filtration rate; DRESS, drug rash with eosinophilia and systemic symptoms; SJS, Stevens–Johnson syndrome; TEN, toxic epidermal necrosis.
Delayed clearance of oxypurinol correlated with poor prognosis of allopurinol-SCAR
Among allopurinol-SJS/TEN, the deceased patients displayed significantly higher concentrations of plasma oxypurinol for a longer period (regression equation: y=7.14−0.429x; R=0.697, n=8) than the survivals (y=1.81−0.025x; R=0.083, n=14) (p=0.005) (figure 3A). The average levels of plasma oxypurinol were significantly higher in the deceased cases of SJS/TEN than the survival patients after allopurinol withdrawal for 0–3 days (6.9±1.2 vs 1.6±0.4 mg/L, p=0.008) or 4–7 days (4.4±0.8 vs 1.6±0.7 mg/L, p=0.034) (figure 3B).

Correlation between the levels of plasma oxypurinol and prognosis of allopurinol-severe cutaneous adverse reactions. (A) Regression equations of oxypurinol levels corresponding to the time after allopurinol withdrawal in survived (n=14) or deceased (n=8) patients of allopurinol-SJS/TEN. (B) The average concentrations of oxypurinol detected at different time intervals after allopurinol withdrawal in allopurinol-SJS/TEN. (C) Regression equations of oxypurinol levels corresponding to the time after allopurinol withdrawal in patients with allopurinol-DRESS with duration of remission of cutaneous reactions <60 days (n=5) or ≥60 days (n=6). (D) The average concentrations of oxypurinol detected at different intervals after allopurinol withdrawal in allopurinol-DRESS. DRESS, drug rash with eosinophilia and systemic symptoms; SJS, Stevens–Johnson syndrome; Ten, toxic epidermal necrosis.
In the allopurinol-DRESS group, patients with longer remission of cutaneous reactions (duration ≥60 days) showed higher concentrations of plasma oxypurinol (regression equation: y=11.4−1.01x, R=0.58, n=6) than those with short remission duration (y=2.33−0.051x, R=0.12, n=5) (duration <60 days) (figure 3C). After allopurinol withdrawal for 0–3 days, the significant higher level of plasma oxypurinol was noted in patients with DRESS with longer duration of completed remission (15.1±5.7 mg/L) than that of patients with short remission duration (1.4±0.6 mg/L) (p=0.029) (figure 3D).
Increased plasma granulysin correlated with renal impairment, mortality and high oxypurinol levels of allopurinol-SJS/TEN
After allopurinol withdrawal (ie, usually the date of SCAR onset and recognition of allopurinol as the culprit drug), concentrations of plasma granulysin were noted to be higher and sustained longer in patients with SJS/TEN with renal impairment (mean granulysin: 342 ng/ml) compared with those with moderate to normal renal function (granulysin <40 ng/mL) (p<0.05) (figure 4A, B). Granulysin level was also associated with the mortality of SJS/TEN, in which the deceased patients showed higher concentrations of granulysin for a longer time (y=649−52.8x; R=0.509) than that of the survivals (y=69.3−3.09x; R=0.278) (p<0.05) (figure 4C, D). Figure 4E illustrates the data of plasma granulysin and oxypurinol levels in patients with SJS/TEN with different renal function. Consistent with the trend of oxypurinol, the concentrations of granulysin were high and persisted for up to 2 weeks after allopurinol withdrawal in patients with SJS/TEN with eGFR <30, whereas lower levels were found in patients with eGFR ≥30 (figure 4E). Six of our tolerant controls (three with eGFR <30, three with eGFR ≥30) were able to discontinue allopurinol therapy and provided their samples to measure the levels of plasma granulysin and oxypurinol after allopurinol withdrawal. Figure 4F shows the comparison of average plasma levels of oxypurinol and granulysin in patients with SCAR (n=18) and in tolerant controls (n=6) at 0–3 days after allopurinol withdrawal. Delayed clearance of oxypurinol was observed in the subjects with renal impairment in patients with SCAR and in tolerant controls (figure 4F). Granulysin is significantly increased in patients with SCAR but not in tolerant controls (figure 4F).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation of granulysin levels with the renal function, mortality and plasma oxypurinol in patients with allopurinol-SJS/TEN. (A) Levels of plasma granulysin measured at 0–14 days after allopurinol withdrawal in patients with different renal function. (B) The average concentrations of granulysin at different time intervals after allopurinol withdrawal in patients with different renal function (eGFR ≥30 or <30 mL/min/1.73 m2). (C) Levels of plasma granulysin measured at 0–14 days after allopurinol withdrawal in deceased or survived patients. (D) The average concentrations of granulysin at different time intervals after allopurinol withdrawal in deceased or survival patients. (E) Levels of plasma granulysin and oxypurinol measured at 0–14 days after allopurinol withdrawal. Data were obtained from 10 patients with impaired renal function (eGFR <30 mL/min/1.73 m2) and 10 with eGFR ≥30 mL/min/1.73 m2. (F) The average concentrations of plasma oxypurinol and granulysin measured at 0–3 days after allopurinol withdrawal in patients with SJS/TEN (n=18) and tolerant controls (n=6). eGFR, estimated glomerular filtration rate; SJS, Stevens–Johnson syndrome; TEN, toxic epidermal necrosis.
Discussion
Previous reports suggest the risk factors of allopurinol hypersensitivity include renal impairment, coadministration of diuretic agents and excessively high and/or rapidly escalated initial allopurinol dosing.17 ,20–23 ,32 ,33 In this study, we did not find higher starting dosage of allopurinol in patients with SCAR, but demonstrated that renal impairment is a risk factor for allopurinol-SCAR. When the starting dose of allopurinol is further divided by eGFR, it indeed showed a significant difference between allopurinol-SCAR and tolerant control, suggesting that renal function should be the major contributing factor. Furthermore, we found renal impairment also correlated with delayed clearance of plasma oxypurinol and high levels of granulysin, all of which had further detrimental effects on the prognosis of allopurinol-SCAR. As SCAR developed in patients early in the course of allopurinol therapy (mean 31 days), this study does not mean that higher concentration of oxypurinol in subjects tolerating and responding to allopuriol is a risk factor for allopurinol-SCAR.
Since more than 97% of oxypurinol is excreted by the kidney and unchanged in the urine, renal dysfunction has been suggested to reduce oxypurinol clearance.34–36 In healthy subjects, the elimination half-life of oxypurinol was reported to be approximately 18–30 h36 or 1 day.15 By comparison, in patients with substantial renal impairment, plasma oxypurinol accumulated and could be detected after 1 week from allopurinol withdrawal.15 ,36 In this study, the levels of plasma oxypurinol remained detectable 2 weeks after allopurinol withdrawal in patients with SCAR with renal impairment, demonstrating the impact of kidney function on the clearance of oxypurinol. The association between high levels of oxypurinol and poor prognosis of allopurinol-SCAR may be explained by the concentrations-related antigenic property of oxypurinol that can induce cytotoxic T-cell response and trigger hypersensitivity reactions in SCAR.16
This study illustrated that in addition to HLA-B*58:01 as a risk factor, the renal impairment and delayed clearance of oxypurinol were the poor prognostic factors of allopurinol-SCAR. The HLA-B*58:01 allele is strongly associated with allopurinol-SCAR, and the ethnic difference of HLA frequency may contribute to the prevalence of the associated disease.10–14 ,37–40 Epidemiological studies showed a high frequency of HLA-B*58:01 in the populations of Southeast Asia, such as Taiwan and Thailand, but a lower prevalence of the allele in Europeans and Japanese.10–14 ,37–40 Moreover, since the incidence of end-stage renal disease in Taiwan is the highest in the world (about 1.35/100 person-years)41 and the allopurinol use is a common treatment for hyperuricaemia in patients with CKD,42 a higher mortality of allopurinol-SCAR was observed in patients with CKD in this study. Our analysis showed that renal impairment and the high concentrations of plasma oxypurinol correlated with the poor prognosis of allopurinol-SCAR, suggesting that delayed excretion of oxypurinol may cause the accumulated toxicity and generate irreversible deterioration to the prognosis of the disease. Further studies are needed to clarify whether early intervention to increase plasma oxypurinol clearance and remove the antigenic oxypurinol, such as by haemodialysis, improves patients’ recovery from allopurinol-SCAR.
Granulysin is responsible for widespread keratinocyte apoptosis in SJS/TEN, and its expression can be induced to reach 50–1000 ng/mL in the plasma at the acute stage of the disease.18 ,19 This study revealed that the levels of plasma granulysin correlated with the renal impairment, mortality and delayed clearance of oxypurinol in allopurinol-SCAR. The corresponding increases of granulysin and oxypurinol indicate that they may have a vicious cycle on disease progression related to the poor and declining renal function and perhaps the retained oxypurinol induces cytotoxic T cell to release granulysin.
In conclusion, this study demonstrated that plasma oxypurinol and granulysin concentrations and renal impairment correlated with the prognosis of allopurinol-SCAR. Potentially, the results provide a rational explanation for the prolonged time to disease remission and high mortality in allopurinol-SCAR. The high and sustained plasma oxypurinol may have antigenic properties to stimulate cytotoxic T lymphocytes, induce granulysin expression and prolong the hypersensitivity reactions, leading to worse outcomes and higher mortality in patients with SCAR with HLA-B*58:01 predisposition. Thus, clinicians treating patients with allopurinol-SCAR with renal insufficiency are suggested to consider alternatives to promote the clearance of plasma oxypurinol, such as haemodialysis, to attenuate the potentially continuous immune stimulation. Whether such an intervention may improve the prognosis of allopurinol-SCAR needs further investigation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
W-HC and W-CC contributed equally.
Contributors WHC: conception and design, collection of study materials and patients’ enrolment, analysis and interpretation of data, drafting of the manuscript. WCC, CJC and YJL: analysis and interpretation of data, statistical analysis. SLS, CGJ and MHHL analysis and interpretation of data. GGG: critical revision of the manuscript and KMW: critical revision of the manuscript. YCT, KCJ, YJJW and CHY: collection of study materials and patients’ enrolment. ROD: conception and design, drafting and critical revision of the manuscript. SIH: conception and design, analysis and interpretation of data, drafting and critical revision of the manuscript.
Funding Work on this manuscript was supported (or partially supported) by the National Science Council, Taiwan (NSC98-2320-B-010-002-MY3, NSC98-2314-B-182A-027-MY3, NSC101-2320-B-010-072-MY3, NSC101-2321-B-010-027, NSC101-2628-B-182-001-MY3, NSC101-2321-B-182-008, NSC102-2314-B-010-014-MY3); the Taiwan Ministry of Education (Aim for the Top University Plan, National Yang-Ming University); grants from Chang Gung Memorial Hospital (BMRPG290011, CMRPG-290051∼3, OMRPG2C0011, OMRPG2C0021, CLRPG340599).
Competing interests None.
Patient consent Obtained.
Ethics approval Institutional Review Board at Chang Gung Memorial Hospital gave approval for the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Technical appendix, statistical code and dataset available from the corresponding author, who will provide a permanent, citable and open access home for the dataset.