Article Text

Abstract
Background High serum uric acid (sUA) has been associated with increased mortality risks, but its clinical treatment varied with potential side effects. The role of physical activity has received limited attention.
Methods A cohort, consisting of 467 976 adults, who went through a standard health screening programme, with questionnaire and fasting blood samples, was successively recruited between 1996 and 2008. High sUA is defined as uric acid above 7.0 mg/dL. Leisure time physical activity level was self-reported, with fully active defined as those with 30 min per day for at least 5 days a week. National death file identified 12 228 deaths with a median follow-up of 8.5 years. Cox proportional model was used to analyse HRs, and 12 variables were controlled, including medical history, life style and risk factors.
Findings High sUA constituted one quarter of the cohort (25.6%). Their all-cause mortality was significantly increased [HR: 1.22 (1.15–1.29)], with much of the increase contributed to by the inactive (HR: 1.27 (1.17–1.37)), relative to the reference group with sUA level of 5–6 mg/dL. When they were fully active, mortality risks did not increase, but decreased by 11% (HR: 0.89 (0.82–0.97)), reflecting the benefits of being active was able to overcome the adverse effects of high sUA. Given the same high sUA, a 4–6 years difference in life expectancy was found between the active and the inactive.
Conclusions Physical activity is a valuable alternative to pharmacotherapy in its ability to reduce the increases in mortality risks from high sUA. By being fully active, exercise can extend life span by 4–6 years, a level greater than the 1–4 years of life-shortening effect from high sUA.
- Gout
- Epidemiology
- Cardiovascular Disease
Statistics from Altmetric.com
Introduction
The management of asymptomatic hyperuricaemia has been baffling clinicians for decades.1 The evidence has been mounting on the adverse mortality effect of high serum uric acid (sUA).2–11 Many studies showed the independent effect of sUA as a risk factor for all-cause and cardiovascular disease (CVD).2–8 When associated with gout or with renal stone, pharmaco-intervention is clinically indicated.12 However, several reports argued that high sUA may not be a primary target for treatment,1 ,13–16 and in most practices, high sUA did not receive treatment. First, most high sUA is asymptomatic but when pharmacotherapy is instituted, substantial side effects from medication could occur, including Steven–Johnson syndrome.17 ,18 Thus, the potential harms may not justify its benefits. Second, high sUA, not considered as a major CVD risk factor, is often accompanied by comorbidities such as hypertension or diabetes.1 Treating these major CVD risk factors could be more important or more urgent than treating high sUA per se.12 ,19 ,20 As a result, the field of managing high sUA is a mixed bag of different reactions from clinicians: Most ignored high sUA and left it unattended. Others offered treatment with medicines, with occasional side effects that could outweigh the benefits. Nevertheless, treating high sUA with medicines is popularly requested by patients. The reality is, however, other than the potential side effects of medication, such a treatment requires a long-term commitment, with the risk to benefit ratios uncertain.
The benefits of physical activity are legion, including the sensation of well-being, extending life expectancy, and reducing mortalities.21 ,22 In order to accomplish this, the prevailing thinking is it requires meeting the exercise recommendation by spending 150 min or more per week on activities of moderate intensity.23 ,24 However, our recent study reported significant beneficial effect from less than the recommended amount.22 A daily physical activity lasting 15 min or more could achieve a 14% mortality risk reduction and extend a 3-year life expectancy.22 Such a short duration made less acceptable the excuses of ‘too busy’ to exercise.
The objective of the study is to assess whether being physically active is associated with reduction of the excess mortality from high sUA. We compared, within a large cohort, study between those active and inactive individuals with high sUA, with or without comorbidities. Given the current uncertainty in treating high sUA, an important objective is to assess whether physical activity could be recommended as part of clinical routine for those with high sUA.
Methods
Study population and follow-up
The detailed information of the study population has been reported elsewhere.22 ,25 In short, we observed 467 976 participants, aged 20 years and older, recruited successively between 1996 and 2008 in a standardised medical screening programme. The screening clinics were operated by a private firm (MJ Health Management Institution) which attracted paying individuals from all over Taiwan. Vital status was ascertained through linking the unique ID of the cohort with the National Death File. As of the end of 2008, 12 228 deaths were identified in a cumulative 13-year follow-up of mortality and 3.5 million person-years of observation. The causes of death were classified according to ICD-9.
An informed consent from each individual, authorising processing and analysis of the data was obtained, and ethical reviews were approved by the Institutional Review Boards at China Medical University Hospital, Taiwan.
Questionnaire and laboratory procedures
Each participant completed a detailed questionnaire containing medical history, lifestyle and demographic information, including education, smoking, drinking and physical activity. Three multiple choice questions were asked to ascertain an individual's leisure time physical activity level, with details reported earlier.22 The duration and intensity of weekly physical activity were converted into MET-hour/week, which was based on Ainsworth's compendium of physical activities.26 Majority of those inactive individuals reported no leisure-time physical activity, with a small group (12.5%) having limited exercise with less than 1 hour per week. Those classified as ‘fully active’, with ≧7.5 MET-hour/week, met the current exercise recommendation of ≧150 min/week, and ‘low active’ exercised 90 min a week on average, or 15 min a day. MET (Metabolic Equivalent for Task) is a unit for exercise intensity with 1 MET=the energy (oxygen) used by the body at rest, while sitting quietly. Activity that burns 3–6 METs is moderate intensity, while activity >6 METs is considered vigorous.
Fasting blood samples were collected and centrifuged and serum was assayed by using Hitachi 7150 autoanalysers (Tokyo, Japan). Obesity was defined with Body Mass Index (BMI) ≧30 kg/m2. Hypertension was identified by medical history, or self-reported antihypertensive drugs use, or positive screening results (systolic pressure ≧140 mm Hg). Diabetes was defined by medical history or self-reported hypoglycaemic drugs use or positive screening results (fasting blood glucose concentration ≧126 mg/dL). Hyperlipidaemia was defined by medical self-reported lipid-lowering agents use, or positive screening results (cholesterol ≧240 mg/dL). High triglycerides was defined as triglycerides ≧200 mg/dL. Antihyperuricemic drugs information was accessed by self-reported. The definition of metabolic syndrome was based on ATP III guideline,27 and the classification of chronic kidney disease (CKD) was based on KDOQI28 with CKD-EPI modification.29 Abnormal liver function was defined as alanine aminotransferase (ALT) or aspartate aminotransferase (AST) ≧80 IU/L.30
sUA was assayed by the colorimetric uricase-peroxidase system.31 In males and females, ‘high sUA’ is defined as ≥7.0 mg/dL. Most medical test data were available except for a few specific elements: educational levels (4.3% missing), smoking (7.4% missing), or drinking (8.2% missing).
Statistical analysis
The Cox proportional hazards assumption was fulfilled for all factors as shown by parallel lines of log (-log(mortality)) versus log of mortality times. Subjects with sUA at 5.0–5.9 mg/dL, were used as the reference group, as they had the lowest all-cause mortality among men and women.
HRs were adjusted for 14 variables in multivariate model with continuous variables whenever appropriate: sex, age (continuous), education levels, smoking (never, ex-smoker and current smoker), drinking (never, occasional and regular) with regular drinking at least three times a week and two drinks each time, systolic blood pressure (continuous), fasting glucose (continuous), total serum cholesterol (continuous), triglycerides (continuous), BMI (continuous), CKD, abnormal liver function, history of heart disease and current takers of uric acid medications. The time at entry was the date of recruitment, and the time of exit was the end of follow-up (Dec 31, 2008) or date of death, whichever came earlier. We used the Chiang life-table method to calculate and compare life expectancy.32 ,33 All statistical tests used p value <0.05 (two-sided) to consider statistically significant. Analyses were done with SAS, V.9.2.
Results
Table 1 shows demographic characteristics of the cohort, by sUA levels. With a total of 467 976 (224 010 men and 243 966 women) participants, one quarter (25.6%) had sUA above 7.0 mg/dL. High sUA were associated with male gender, elderly, smokers, alcohol drinkers, physically active, hypertensive, high cholesterol, obese individuals (BMI≧30 kg/m2) and abnormal liver function (ALT or AST≧80 IU/L). High sUA had higher prevalence of metabolic syndrome, CKD, including reduced eGFR and proteinuria. Among the high sUA group (≧7.0 mg/dL), approximately half (49.7%) were inactive, and one quarter (28.1%) met the current recommendation for leisure-time physical activity.22
Demographic characteristics and conventional and non-conventional risk factors for the cohort by sUA levels
Online supplementary figure S1 shows the mean sUA levels, decreasing from 7.0 to 6.7 mg/dL from age 20 to 80 years for males, but, for females, increasing after age 45 years, from 5.0 to 6.2 mg/dL. Mean levels in females remained lower than males throughout. High sUA (≧7.0 mg/dL) was more common for males than females, with 40.4–48.5% for males and 5–22.7% for females.
All-cause mortality risks (HR) increased among high sUA when compared against normal values of 5–5.9 mg/dL, with 22% increase for the entire cohort, by adjusting for 12 confounders. A 27% increased mortality was found among the inactive with high sUA when compared with 5–5.9 mg/dL (table 2). Mortality risk for each sUA level above 6 mg/dL of the inactive was significantly increased. Among those fully active, the 27% increases in mortality risks of inactive subjects disappeared, in addition to showing 11% significant reduction (HR=0.89), a swing of 38% by converting from inactive to active (figure 1). With additional adjustment of non-conventional risk factors such as CKD, or abnormal liver function, the increased HRs were attenuated from 1.27 to 1.14 for high sUA among the inactive, but the benefits of exercise remained or increased from 11% (0.89) to 19% (0.81). As all HRs remained significant, we chose the HRs adjusted with conventional risk factors for the rest of the study. For the low active, mortality increases also largely disappeared.
All-cause mortality risks by sUA levels and by physical activity status

Mortality risks by physical activity status among individuals with high sUA.
The beneficial effect of physical activity on selected risk factors in high sUA subjects is shown in figure 2 forest plot and Table S1. When the risk factor was examined one at a time, the effect of physical activity in reducing mortality was significant for either with or without risk factors. When two risk factors coexisted, such as smoking and CKD or diabetes and hypertension, being fully active significantly reduced the mortality risks. The differential effect of physical activity persisted regardless of severity of comorbidity, such as levels of fasting glucose or systolic blood pressure.

Beneficial effects of physical activity by risk factor/comorbidity among high sUA subjects. Reference group was inactive subjects with high sUA, hazard ratios were adjusted by 14 confounders: sex, age, education, systolic blood pressure, fasting glucose, BMI, total cholesterol, triglycerides, CKD, abnormal liver function, smoking, drinking, history of heart disease, and antihyperuricemic drugs for all-cause mortality among those fully active compared with those inactive in high sUA HR for the entire cohort was 0.74 (0.68–0.80). A, hyperlipodemia was defined as cholesterol ≧240 mg/dL, or use of lipid-lowering agents use; B, high triglycerides was defined as triglycerides ≧200 mg/dL; C, obesity was defined as BMI≧30 kg/m2; D, the definition of metabolic syndrome was based on ATP III; E, the classification of CKD e was based on the KDOQI clinical practice guideline; F, proteinuria was defined as any amount of proteinuria detected by dipsticks, including trace, 1+ and above; G, eGFR was estimated by using CKD-EPI and reduced eGFR defined as eGFR<60 mL/min/1.73 m2; H, abnormal liver function defineded as ALT≧80 U/L or AST≧80 IU/L; I, diabetes was defined as fasting glucose ≧126 mg/dL, history of diabetes, or use of diabetes drugs; J, hypertension was defined as systolic BP≧140 mm Hg, history of hypertension, or use of hypertension drugs.
Inactivity among high sUA shortened life by 4.3 years in males and 5.7 years in females, while high sUA shortened 1.4 and 3.8 years, in males and females, respectively, when compared with normal uric acid (figure 3 and Table S2).

Comparison of life-shortening effect among high sUA subjects. High sUA was defined as serum uric acid ≧7.0 ug/dL. †Difference of life expectancy between sUA 4.0–6.9 ug/dL and high sUA. φDifference of life expectancy between fully active and inactive among high sUA.
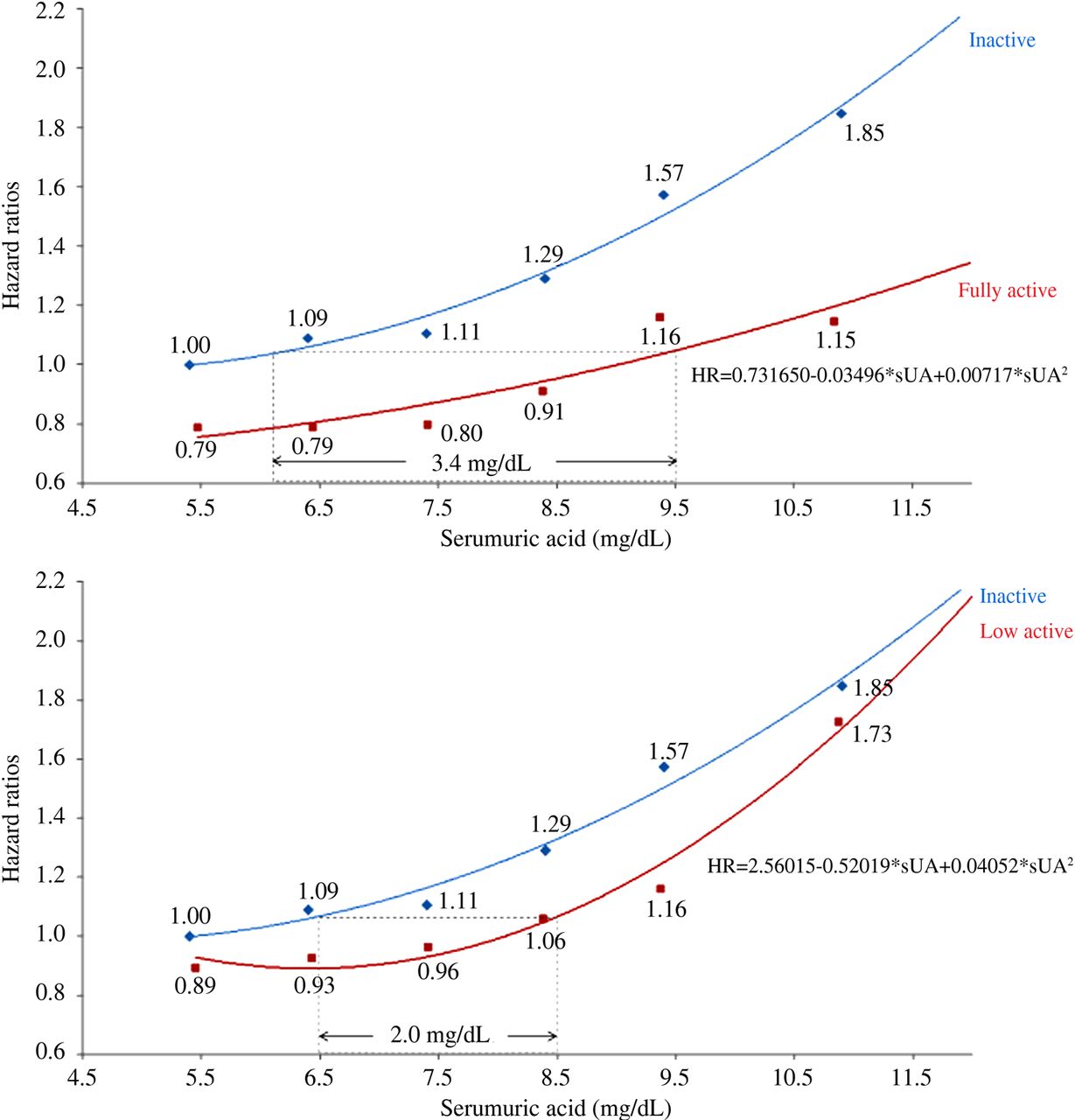
The size of mortality reduction of the fully active could be translated and expressed in sUA equivalent by fitting a line through a hazard ratios graph. Fully active reduced the risks of all-cause mortality by an amount equivalent to the mortality reduction from reducing sUA by 3.4 mg/dL, and the low active, equivalent to reducing 2.0 mg/dL (figure 4, and see online supplementary table S3).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Translating the benefits of exercise into uric acid equivalent, based on reduction of mortality by being fully active. The all-cause mortality risks at all-serum uric acid levels for the inactive, low active and fully active, were plotted in online supplementary figure S1. We fit a quadratic regression line, R=a+b1x+b2x2 based on the HRs for the active, where x is the serum uric acid value of the active group. The fitted line yielded HR=0.731650–0.03496*sUA+0.00717*sUA2 for the fully active (A), and HR=2.56015–0.52019*sUA+0.0.04052*sUA2 for the low active (B). For any given mortality risk of the inactive with equivalent uric acid, the same mortality risk for a fully active individual, but with uric acid, could be identified. For example, as shown in the supplementary table 3, when HR in the inactive was 1.00 with its uric acid being 5.4 mg/dL, we can find the corresponding uric acid with the same HR in the fully active group by solving the equation: 1.00=0.731650–0.03496*sUA+0.00717*sUA 2. This resulted in a uric acid of 9.0 mg/dL for the fully active. This implied that, while this inactive individual had a uric acid at 5.4 mg/dL, his inactivity gave him an additional mortality risk equivalent to 9.0 mg/dL when compared to the fully active, an increase in risk equivalent to 3.5 mg/dL. On average, by weighing the distribution across the uric acid range, inactivity as a whole was equivalent to an increase of 3.4 mg/dL for the inactive individuals.
Discussions
This study demonstrated the beneficial effect of physical activity to reduce or eliminate the 27% increase and to add 11% decrease in all-cause mortality risks by those fully active among high sUA subjects (≧7.0 mg/dL). By being fully active, those with high sUA extended their life expectancy by 4–6 years, a level far more than the 1–4 years of life-shortening effect from high sUA. The experience of the high sUA but fully active group was noteworthy. First, all the adverse mortality risks of high sUA were modified among those fully active. Second, the beneficial effect of physical activity was consistently similar between those with comorbidities and those without comorbidities in high sUA subjects, reflecting its independent effect among 13 risk factors (figure 2). Third, when compared to the inactive group with normal sUA (5.0–5.9 mg/dL), fully active ones showed better mortality experience, including an advantage of up to 11% (HR=0.89, 95% C.I 0.82 to 0.97) over and above normal sUA group but physically inactive. In other words, being fully active potentially overcame the hazards of high sUA and more. Physical exercise was a valuable factor able to reverse the increases in mortality associated with high sUA, and also to gain additional benefits and to extend life span. In the clinical management of high sUA, if physical activity were compared with pharmacotherapy, becoming fully active may be as effective as taking medication, if not more. By contrast with pharmacotherapy, exercise is inexpensive and free from known side effects. Benefits were seen for all-cause as well as CVD mortality, from physical activity (Table S1).
The ‘fully active’ individuals exercised, on average, 150 min a week or 30 min a day for five or more days a week, at moderate intensity, a level currently recommended by numerous organisations.22–24 While this is a desirable goal to pursue, we found that those who exercised minimally, like 15 min a day instead of 30 min, in brisk walking instead of jogging, also had reduced nearly all mortality increases from high sUA. Clinicians rarely give an ‘exercise prescription’ to patients with high sUA, as ‘exercise prescription’ sounds complex and technical. However, counselling those with high sUA for a daily routine of 15 min of exercise, starting with brisk walking, is a task simple enough for physicians to perform. Many physicians are reluctant to treat high sUA with medications, and leave patients with risks unattended. This may not be desirable. In this regard, counselling with physical activity can be an acceptable alternative and could be considered as part of the clinical practice guidelines.
In clinical trials, strenuous exercise was known to increase production of sUA, leading to slightly higher serum levels temporarily.34 Uric acid, a water-soluble antioxidant, is said to increase during exercise and reflects enhancement of antioxidant defences as a response to oxidative stress of exercise.35 ,36 However, the amount of sUA produced is related to whether the exercise is strenuous or not. Light regular exercise would only produce minimal elevation of sUA levels compared to heavy exercise.37 A recent cross-sectional study on elderly Chinese women found that daily exercise was inversely related to the prevalence of hyperuricaemia, in a dose-response manner, supporting the notion that exercise may have a direct effect on sUA levels in the long run.38
Whether exercise per se was able to reduce sUA may be a moot point, once we recognise the sustaining and highly beneficial effect of exercise on the outcome of long-term mortality.22
To facilitate counselling exercise in the high sUA patient, we developed ‘sUA equivalent’ for physical activity (figure 4 and see online supplementary table S3). Patients will pay more attention when exercise benefits were expressed in sUA equivalent. Fully active was equivalent to a mortality reduction of sUA by 3.4 mg/dL. This reduction of sUA equivalent can be achieved by exercise without medication. Furthermore, the benefits can be long-lasting, unlike the temporary nature of pharmacotherapy. In short, reducing sUA equivalent of 3.4 mg/dL by being fully active, and 2.0 mg/dL by being low active, physicians can initiate a discussion on exercise benefits.
The prevalence of hyperuricaemia defined as 7.0 mg/dL or more has been reported as high as one third in parts of Asia,39–42 but nearly one quarter in the USA,43 similar to 25.6% in this study. On the other hand, gout was far rarer with 0.1–0.6% in Taiwan.44 ,45 Thus, high sUA associated with increased mortality is a global phenomenon, affecting one quarter to one third of the population, and our recommendation to use physical activity to attenuate such a risk has far-reaching implications, in saving lives as well as in improving quality of life.
There had been concerns about the potential bias that active people were healthier to begin with, and the inactive were sicker with more comorbidities and risk factors. Some explanations already appeared in the original Lancet article,22 but more elaborations are in order here. First, we controlled as many as 12 confounders in the Cox analysis, so the exercise effect should be independent of these comorbidities. Additionally, the large size of the resulting HR after adjustment showing the exercise effect, 0.89 or 11% benefits on top of reversing 1.27 or 27% hazards of high sUA, and the presence of a strong dose-response relationship strengthened our argument favouring the active role of physical activity. Second, we addressed those with risk factor, or comorbidity, not necessarily healthier to start with, in figure 2, and confirmed the significant benefits of being active for those less healthy individuals with one of the 13 risk factors. Beyond these 13 risk factors, we also looked at two risks coexisting at the same time, such as smoking and CKD, or diabetes and hypertension, as an example, and found the significant benefits remained. When levels of severity of some comorbidity were individually examined, such as levels of fasting glucose or systolic blood pressure, differential effect of physical activity persisted (figure 2). In this way, we looked at less healthy subjects with high sUA, regardless of whether they had one, two or multiple comorbidities, or regardless of severity of comorbidity at initial intake, physical activity was beneficial. Third, the effect of exercise is obviously not limited to high sUA, but a systemic effect, by directly acting on those with comorbidities. This is why the health benefits found on those with numerous comorbidities were as large as those without comorbidity. In short, we have produced data to support the direct relationship between exercise38 and health. However, there is a positive interactive vicious cycle, with incremental exercise leading to better health which, in turn, led to more exercise, blurring the conventional cause-and-effect relationship.
As the advice to stress physical activity can be offered to the general public, those with high uric acid will be more receptive and, consequently, benefit more from such advice.
There are important limitations in this study. First, physical activity information came from self-reported history and was not validated. As exercise is a socially desirable behaviour, people may tend to over-report active exercise. For a prospective cohort study, any bias from exercise history should have no bearing on different sUA levels. If the results were diluted by those over-reporting, the exercise benefits we observed would have been underestimated. Second, only the initial sUA was used for this study. While levels of sUA could vary by time, this study, by relying on one single measurement, was able to simplify the relationship and demonstrate the dose response effect between high sUA and mortality risks. Third, some members of the cohort were on medications for sUA, with a possible temporary lowering of sUA. In cases where their sUA levels remained high, the beneficial effect of additional physical activity was demonstrated.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors JHC and CPW conceived the study concept and design. CCH, CKT and CAH investigators and collaborators acquired the data. SBW, MKT, JHL and YPT analysed the data. JHC and CPW drafted the report. JLL, PHC, WHP provided critical revisions for important intellectual content. All authors took part in the interpretation of the data.
Funding This study is supported, in part, by Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH102-TD-B-111–004). The funding source had no role in study design, data collection, data analysis, data interpretation, writing of the report, or in the decision to submit the paper for publication.
Competing interests None.
Patient consent Obtained.
Ethics approval MJ Health Management Institution and at National Health Research Institutes.
Provenance and peer review Not commissioned; externally peer reviewed.