Article Text

Statistics from Altmetric.com
Introduction
Modern rheumatology practice endorses the principle of ‘treat-to-target’, with an aim to achieve sustained remission or low disease activity (LDA) in patients with rheumatoid arthritis (RA).1 This treatment approach results in significant clinical benefits, with improved functional and radiographic outcomes.2–6 The majority of RA patients will achieve this goal with disease modifying antirheumatic drugs (DMARDs), but approximately 20–30% of RA patients will go on to require initiation of advanced therapy with biological agents to control their disease.7 ,8
To date, the healthcare service utilisation costs incurred by the Canadian healthcare system with the initiation of biological therapies, and the long term cost benefits, have not been explored. Some of the initial healthcare service utilisation costs to consider include increased physician and allied health professional visits, and baseline investigations prior to receiving treatment. Following therapy initiation, additional follow-up visits to healthcare service providers are necessary to evaluate for treatment effectiveness and any adverse events. Given that there is significant potential to improve patient outcomes with good disease control, long-term healthcare service utilisation costs associated with hospitalisations, surgeries or medical visits to treat complications caused by progressive disease may be reduced. This reduction may be particularly noticeable in those patients who are able to achieve and maintain the lowest levels of disease activity or remission with effective treatment.
In 2004 the Alberta Government funded a pharmacosurveillance programme (The Alberta Biologics Pharmacosurveillance Program, ABioPharm) for all publicly funded RA patients receiving biological therapy to monitor treatment efficacy, safety and economic consequences.9 This programme, a unique partnership between the Divisions of Rheumatology at the Universities of Calgary and Alberta, government, and industry in our province, has enabled the examination of healthcare service utilisation costs and clinical outcomes for patients using biological therapies. The specific premise of this paper is to examine healthcare service utilisation costs associated with RA treatment using biological therapies, considering physician billing claims, outpatient department visits and hospitalisations, taking into account the magnitude and duration of patient response achieved over a 5 year period of observation.
Methods
Data sources
The Alberta Biologics Pharmacosurveillance Program (ABioPharm) was initiated in 2004 to identify the efficacy, safety and cost effectiveness of new biological therapies for RA.9 Patients in Alberta qualify for anti-tumour necrosis factor (TNF) therapy cost coverage if they have RA refractory to parenteral methotrexate, in combination with at least one other DMARD, and leflunomide. They must achieve and retain a minimum DAS28 improvement of 1.2 units and a minimum improvement of their Health Assessment Questionnaire (HAQ) score by 0.22 units over their baseline scores at 12 weeks to continue receiving cost coverage for anti-TNF therapy. Patients who fail to meet these response criteria will be switched to another anti-TNF therapy or a biological therapy with a different mechanism of action. Patients participating in the programme are assessed for disease activity, adverse events, impact on function and quality of life, healthcare utilisation and self-reported economic impact of their disease at the start of a new biological agent, 12 weeks after initiation of that drug, and at 6 month intervals if no treatment switches have occurred. The patients are also brought in for assessment if they contact the programme reporting suspected treatment failure or adverse events which may require a treatment switch.
Clinical data from ABioPharm was linked with provincial administrative databases maintained by Alberta Health and Wellness to identify health services utilisation and associated costs of the RA patients. Datasets available include physician billing claims, outpatient department and emergency room visits (Ambulatory Care Classification System, ACCS), and hospitalisations (Discharge Abstract Database). Clinical data and provincial administrative data collected between 1 April 2004 and 31 March 2009 were used in our analysis.
All patients provide informed consent in accordance with ethical standards described in the Declaration of Helsinki. The study is approved by the University of Calgary Health Research Ethics Board and by the University of Alberta Research Ethics Board. The programme is supported by a grant through Alberta Health and Wellness.
Analysis categories
Disease activity status was determined using DAS28 scores.10 As we wanted to specifically consider costs associated with sustained levels of disease activity, we identified the best DAS28 achieved, and the continuous length of time this level was sustained. Thus, we identified patients achieving DAS28 remission (≤2.6), LDA (DAS28>2.6 but ≤3.2) or persistent moderate or high disease activity (>3.2) for time periods of ≤1 year and >1 year.
Healthcare service utilisation costs determination
We estimated both the annual mean and median healthcare service utilisation costs per patient for each category of disease activity and duration for the entire study period as well as individual fiscal years. All services and procedures provided during hospitalisations and emergency room visits, or ambulatory care contacts including same-day surgery, day procedures and community rehabilitation programme services occurring in publicly-funded facilities, were considered, and are those paid entirely by Alberta Health and Wellness or Regional Health Authorities. The cost of each inpatient stay was estimated by multiplying the Alberta average inpatient cost (derived from the provincial Management Information System data) per patient-day by the length of stay. The cost of each outpatient visit was estimated by the average unit cost corresponding to the ACCS grouper code assigned to the visit. Physician billing claims for all patient encounters whether in hospital or the emergency room are also provided per individual. Additionally, we attributed costs as RA-related or not RA-related, determined by consensus of four rheumatologists (CB, JH, LM and WPM) who reviewed all the International Classification of Diseases (ICD) 9 and 10 diagnostic codes associated with physician billing claims, ACCS and Discharge Abstract Database datasets. RA-related costs were those directly associated with musculoskeletal disease, extra-articular manifestations, recognised comorbidities such as cardiovascular disease and osteoporosis, and potentially treatment-related complications such as gastrointestinal ulcerations, infections and malignancy. Non-RA related costs were those encounters deemed not to be directly related to RA or its recognised complications, and included visits for endocrine, allergic or psychiatric conditions, or genitourinary or gynaecological disease. We used a kernel propensity score matching technique11–13 to compare the mean cost differences between disease activity categories. Propensity score matching identifies similar characteristics between subjects in each disease activity category, and compares the costs of these sets, to imply that differences can be attributed to the disease activity state and not a confounder. Our propensity score matching technique accounted for confounding by variables affecting healthcare utilisation, including specific therapy received, smoking status, age, sex, baseline function measured by the HAQ score, disease duration and medical comorbidities. We used a bootstrap method to estimate 95% CIs of the differences between disease remission categories. Quantile regression was performed to calculate the median cost differences accounting for the same confounding factors.
Stata MP 11.2 (StataCorp, 4905 Lakeway Drive, College Station, Texas, USA) was used for analyses. All the costs were converted to 2008 Canadian dollars using the Canadian Consumer Price Index.
Results
Our cohort includes 1086 RA patients treated with anti-TNF therapy enrolled in ABioPharm between 1 April 2004 and 31 March 2009. The cohort is described in table 1. Given that there were few patients with a LDA period lasting >1 year (n=35) we were unable to evaluate this group with any certainty.
Alberta biologics pharmacosurveillance program patient characteristics, 2004–2009
The largest cost was related to hospitalisation, with a total annual crude mean cost of $2349 for all disease response categories and durations, although notably the non-RA related costs of hospitalisation were almost sixfold higher in the patients with moderate or high disease activity relative to patients in sustained remission ($2264 vs $401) (figure 2). The second largest cost was related to physician visits, with higher costs incurred by the persistent disease activity group ($782 for RA-related and $1306 for non-RA related physician visits) relative to the sustained remission group ($499 for RA-related and $838 for non-RA related physician visits) (table 2). Costs directly attributable to RA-associated visits or conditions were constant across all disease activity categories, accounting for approximately 30% of mean healthcare costs.
Mean annual crude costs (SD) incurred by rheumatoid arthritis patients on biological therapy, by disease activity response and duration, in 2008 Canadian dollars
We note that these differences remained significant when evaluating median costs. The crude median total healthcare service utilisation costs for patients remaining in moderate or high disease activity was $3253 annually, with a savings of $698 (95% CI 121 to 1276, p=0.018) for patients with a DAS28≤2.6 for ≥1 year, and $541 (95% CI 100 to 982, p=0.016) for patients with a DAS28≤2.6 for <1 year. Even a brief period of LDA was beneficial, with a savings of $664 (95% CI 83 to 1245, p=0.025).
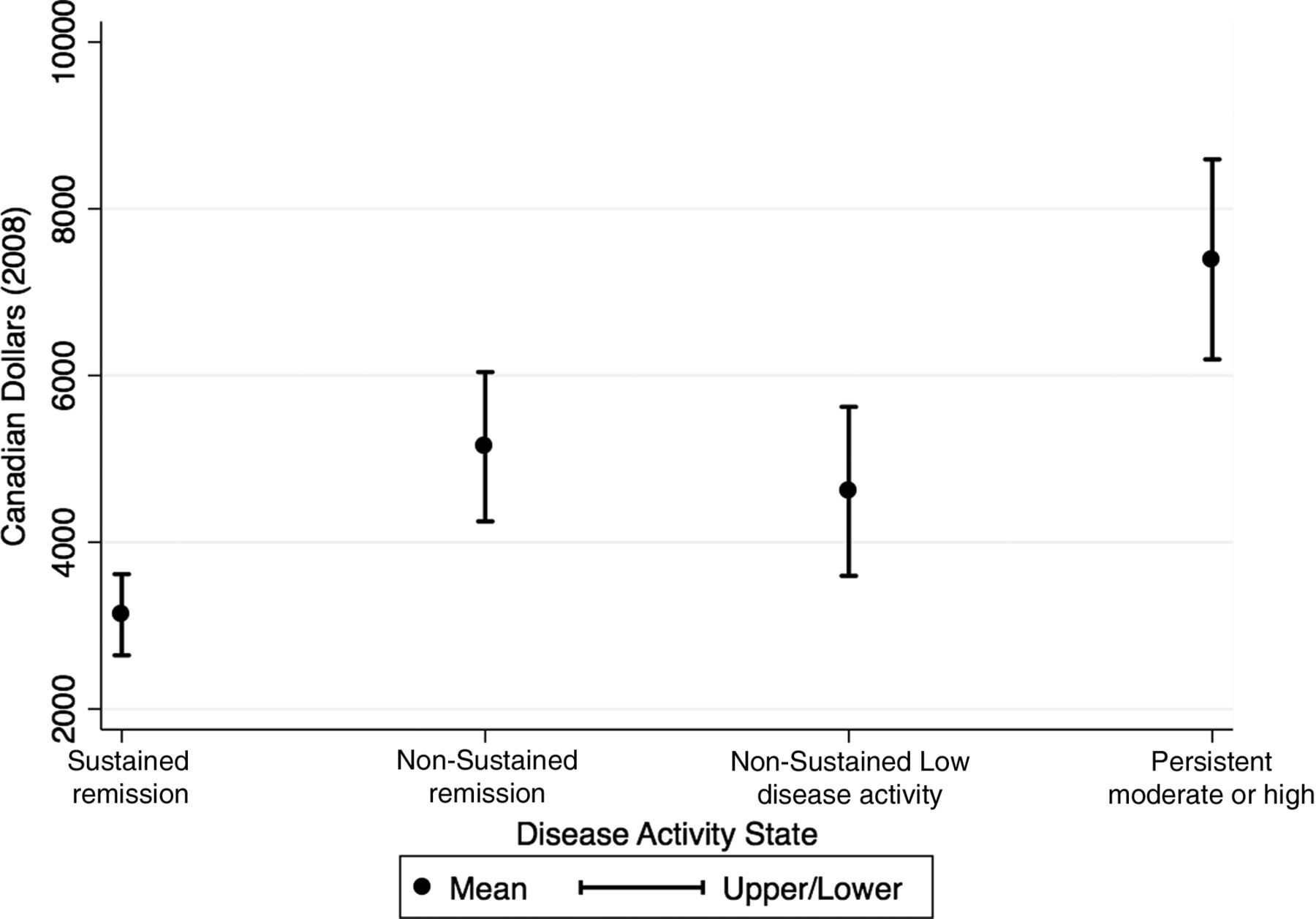
After adjustment for specific therapy received, smoking status, age, sex, baseline HAQ score, disease duration and medical comorbidities, patients achieving sustained remission had the greatest reduction in healthcare service utilisation costs, relative to those patients who had persistent moderate or high disease activity (figure 1; quantile regression coefficients appear in online supplementary table S1). Patients with a DAS28≤2.6 for ≥1 year compared to those with a persistent DAS28 score of >3.2 had a mean annual healthcare cost savings of $2391 (95% CI 1437 to 3909, p<0.001). We also observed system savings for those achieving sustained remission compared to those whose remission period was not sustained. The mean annual cost savings per individual patient achieving a DAS28≤2.6 for ≥1 year was $1422 (95% CI 564 to 2796, p<0.001) compared to those patients with a DAS28≤2.6 for <1 year. We did identify significant cost savings for the group of patients achieving only a brief period of LDA (DAS28>2.6 but ≤3.2 for <1 year) relative to those remaining in moderate or high disease activity, with a mean annual difference of $2104 (95% CI 838 to 3512, p<0.001).

Total annual mean costs by duration and level of disease activity achieved.
Analysis of healthcare service utilisation costs in each fiscal year of the study did not reveal any trend for change over the 5 years of observation (data in online supplementary table S2). Also, we did not identify any continual improvement in cost savings after the best disease activity level had been achieved. To illustrate, cost savings were observed in the first 6 months after achieving remission, and costs incurred in the first and second 6 months after achieving remission were similar (table 3).
Total crude healthcare costs over time in patients with sustained remission
Discussion
The study provides evidence of economic benefits for the Canadian healthcare system resulting from the achievement of good disease control of RA for patients requiring biological therapy. In particular, the greatest savings are observed for patients achieving sustained remission, but benefits from brief periods of remission and LDA were observed.
A systematic review to inform the EULAR RA management recommendations found anti-TNF therapy to be cost-effective if DMARDs had failed. This review considers both treatment and societal costs using incremental cost effectiveness ratio methodology, which calculates the additional cost per quality-adjusted life-year gained with treatment.14 A recent review by Fautrel et al15 highlights that cost reductions related to health resource use are not specific to biological therapy alone, but reflect the improvement in RA diagnosis and management in recent years. As the majority of our patient cohort has long-standing disease, we did not observe a reduction in healthcare service utilisation costs over the fiscal years during our study, but this may become apparent with further observation.
Few studies have considered treatment response magnitude or duration in examining healthcare system costs in RA. It is apparent from our results that estimates of healthcare service utilisation costs vary by clinical response and the duration of that response. Future health economic analyses should incorporate variables in the model to address the magnitude of treatment effect. This is supported by two other studies. A simulation model analysis from France, not specific to biological therapy, estimated eight resource utilisation items by level of disease activity based on expert opinion, including medical visits, laboratory testing, hospitalisation, imaging, physiotherapy, nursing, adaptive aids and transportation.16 Attaining remission or LDA was associated with substantially lower modelled medical costs. It was estimated that the mean cost for patients achieving remission in the first 6 months was €771, and €511 for each subsequent 6 month period (p<0.001). The mean cost associated with achieving LDA was €905 for the first 6 months and €696 for the subsequent 6 month period (p<0.001). Our data, based on actual patient utilisation, did not find that costs varied beyond the first 6 month period in remission. We also highlight that in the French study, patients not achieving LDA or remission had a mean cost of €1159 per 6 month period,16 which is similar to our cost estimate for that same patient group (1 C$≅1.4 €).
The Swedish TIRA project, an early RA project without a prespecified treatment protocol, collects clinical, laboratory and healthcare use data. Direct and indirect costs are estimated from the clinical and self-report data.17 Costs were compared for the group of patients able to achieve a DAS28 score of <3.2 at 3 months, and those who didn't, over the course of 4 years after inclusion. Significant differences in annual direct costs were found between the two groups for years 1–3 (year 1 mean difference €1387 (p<0.001), year 2 mean difference €726 (p=0.019), year 3 mean difference €1392 (p<0.001)). This analysis did not specifically examine the duration of the initial clinical response achieved.
An interesting observation from our results is that the proportion of the healthcare service utilisation costs attributable to RA is constant across disease activity categories. The variability in costs between disease activity categories is thus ascertained to other medical conditions which are not typically recognised as direct consequences of RA, such as psychiatric disease, endocrine disorders, allergic conditions or genitourinary disorders. This suggests that improved RA control has some measurable effect on comorbid conditions. In particular, for patients who do not achieve LDA or remission, hospitalisations for non-RA related conditions accounted for the largest proportion of all healthcare service utilisation costs.
We acknowledge there are some limitations of our work. We have assumed that the levels of disease activity evaluated at 6 month consecutive time points represent a stable period in a particular disease activity state, whereas in reality patients may have experienced limited flares during that time. Any patients contacting the programme to report an increase in disease activity between these 6 month time points would have been assessed for treatment failure and their disease activity scores recorded. An ‘area under the curve’ approach to evaluate longitudinal disease activity would be ideal, but not feasible in the setting of standard clinical care. We did perform a sensitivity analysis to evaluate costs by disease activity state durations of 6 months, 1 year and 2 years, and selected the 1 year time period to ensure that the disease activity period has stabilised and that statistically we could demonstrate our conclusions with confidence, as few patients had sustained remission for a time period of at least 2 years.

{kind=link}
{kind=link}
Total and categorised costs by disease activity state.
We have used provincial data that captures all publicly funded services to determine healthcare service utilisation costs. The cost of privately funded services such as chiropractic treatments, massage therapy and private mental health services were excluded from the study. We have not included costs associated with patient communication by healthcare providers by telephone or email. During the period of this study, some Alberta rheumatologists were enrolled in an alternative relationship plan, which provides salaried income. This plan does mandate that physicians continue to report all patient care encounters, but given that income was not dependent on this, there may be under-reporting of clinical activities and thus costs. An additional limitation is that we did not have access to prescription drug data, although we would expect that these excluded costs would follow the same pattern as healthcare service utilisation costs. These identified issues would result in underestimation of the annual healthcare service utilisation costs for all patients, as well as underestimating the difference between disease activity groups if indeed more prescription drugs were needed for patients in the higher disease activity categories.
We have demonstrated healthcare service utilisation cost savings when RA patients achieve good disease control, and in particular if this control can be sustained for long periods of time. Coupled with expected productivity increases with improved RA control, there is a societal benefit to supporting advanced RA management with biological therapies in patients with DMARD-refractory disease.
Acknowledgments
We express thanks to our colleagues, research assistants and nurses in the Divisions of Rheumatology at the Universities of Calgary and Alberta.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Handling editor Tore K Kvien
-
Contributors All authors were involved in study design, data acquisition, data analysis, drafting of the manuscript and approval of the final version for submission.
-
Funding The Alberta Biologics Pharmacosurveillance Program (ABioPharm) was supported by a grant from Alberta Health and Wellness for the study period reported.
-
Competing interests None.
-
Ethics approval University of Calgary Health Research Ethics Board and the University of Alberta Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.