Article Text

Abstract
Objectives This project was undertaken to assess the risk of malignancy in patients with rheumatoid arthritis treated with tumour necrosis factor inhibitors (TNFi) in clinical practice, as recorded in prospective, observational studies.
Methods The authors undertook comprehensive searches of MEDLINE, EMBASE, the Cochrane Database of Systematic Reviews and American College of Rheumatology, European League against Rheumatism and British Society for Rheumatology conference abstracts according to a prespecified protocol.
Results The searches identified 2039 full-text papers and 1979 conference abstracts, of which 21 full texts and eight abstracts met the inclusion criteria. The pooled estimate for the risk of all-site malignancy from seven studies was 0.95 (95% CI 0.85 to 1.05). Two studies reported there was no evidence that longer exposure to TNFi agents increased the risk of malignancy. In patients with previous malignancies there was a higher risk of a new/recurring malignancy. This risk was not increased further by exposure to TNFi, although CI were wide. Results from four studies showed that patients treated with TNFi have a significantly increased risk of developing a non-melanoma skin cancer (1.45, 95% CI 1.15 to 1.76). In addition, patients are at an increased risk of developing melanoma, as the pooled estimate from two studies was 1.79 (95% CI 0.92 to 2.67). The pooled estimate for the risk of lymphoma was 1.11 (95% CI 0.70 to 1.51).
Conclusions This systematic review and meta-analysis shows that TNFi treatments do not increase the risk of malignancy, particularly lymphoma. However, they do appear to increase the risk of skin cancer, including melanoma.
Statistics from Altmetric.com
Patients with inflammatory arthritis, especially rheumatoid arthritis (RA), have an increased risk of developing a malignancy, particularly lymphoma and lung cancer, but have a reduced risk of developing colorectal and breast cancer.1 The effect of treatments acting on the immune system may affect these risks; however, randomised controlled trials (RCT) may be unable to determine the existence of such effects due to the relatively short duration of exposure to treatment and limited patient numbers.
Tumour necrosis factor (TNF) alpha is a key cytokine in the inflammatory cascade. It plays an important role in host defence against infections2 and cancer,3 and was identified as a potential therapeutic target for autoimmune disease.4 Three tumour necrosis factor inhibitors (TNFi) were approved in the early part of the last decade for the treatment of RA, psoriatic arthritis (PsA) and ankylosing spondylitis. Infliximab and adalimumab are monoclonal antibodies (MAb) directed against TNF, whereas etanercept is a fusion protein of human p75 soluble TNF receptor and human IgG1. Differences in kinetics and mode of action between etanercept and the MAb have been reported.5
Recent meta-analyses of clinical trial data reported a significantly increased risk of cancer with adalimumab and infliximab.6 An analysis of pooled individual patient data for etanercept studies by the same group showed a non-significant increased HR compared with controls.7 Registration trials, however, exclude patients with significant comorbidities and so the results may not be generalisable to RA patients as a whole. Indeed, risks may be greater in clinical practice compared with those identified during drug testing due to the presence of these comorbidities.
As a result of these concerns, proposals to establish observational registries to examine the long-term safety of the TNFi in usual clinical care were published,8 9 and were subsequently set up in a number of European countries by the national professional societies or local groups, usually with financial support from the relevant pharmaceutical companies.
The aim of the present work was to perform a systematic review of prospective observational studies in patients with inflammatory arthritides that include malignancy data.
Materials and methods
Search strategies
The authors have undertaken a systematic review of prospective observational studies of TNFi in usual clinical settings. The search strategy was designed to capture such studies that were then evaluated for the outcomes of interest; in this publication we report on malignancy.
In accordance with a prespecified protocol (see supplementary appendix 1, available online only), an experienced medical information specialist conducted comprehensive literature searches using DataStar (http://www.datastarweb.com) of MEDLINE, EMBASE and the Cochrane Database of Systematic Reviews (RH). The search strategy for MEDLINE (MEYY) is available online (see supplementary appendix 2, available online only).
The search (restricted to studies published since 1998) was conducted on 26 January 2009 and updated on 8 March 2010.
The American College of Rheumatology, European League against Rheumatism and British Society for Rheumatology conference abstracts from 2005 were also searched to minimise the effects of publication bias. Those abstracts subsequently published in full text were removed from the review to avoid duplication of data.
Inclusion criteria and procedure
In this report, we included all studies that reported data for malignancies associated with TNFi treatment that: (1) were a prospective observational registry set up for the assessment of outcomes in rheumatology; (2) included patients with RA, PsA or ankylosing spondylitis; (3) included patients receiving TNFi therapy. Only English language studies were included. Studies with less than 100 exposed patients were excluded. Retrospective studies were excluded to minimise heterogeneity. Administrative databases were also excluded as they do not capture disease-specific clinical data and were not set up prospectively with the purpose of analysing outcome data.
Initially, titles and/or abstracts for all identified citations were reviewed independently by two of the authors (RH, CW) (first pass), followed by a second review stage of full-text publications using a recognised method of positive inclusion (RH, CW) (second pass).10 Full details are provided online in the protocol. Disagreements regarding the inclusion of articles were resolved by discussion between all authors.
Following the screening stages, one reviewer extracted data (CW). The data extraction was performed using a similar protocol to Sugiyama et al.11 Data extracted included the study design, patient characteristics and malignancy (all-site, haematopoietic and skin) outcomes. A second reviewer (RH) checked the data extraction in order to ensure accuracy; any inconsistencies were discussed and resolved at this stage.
The Newcastle–Ottawa quality assessment scale12 was used by one reviewer (CW) to assess the quality of the included publications. This tool is designed specifically for non-randomised studies and avoids the reporting of summary scores, which have been shown to be unreliable and difficult to interpret.13
Statistical analysis
Publications that reported incidence rates, standardised incidence ratios (SIR) or measures of RR, such as incidence rate ratios (IRR), OR or HR were selected for inclusion in the meta-analyses. In publications not reporting these statistics, the data were calculated from primary data when available. Direct random effects meta-analyses were conducted using, unless otherwise specified, the most recent data from each source. These meta-analyses were conducted in a frequentist framework using Stata version 11. The level of heterogeneity was determined using the I2 statistic.
Results
Selection of studies
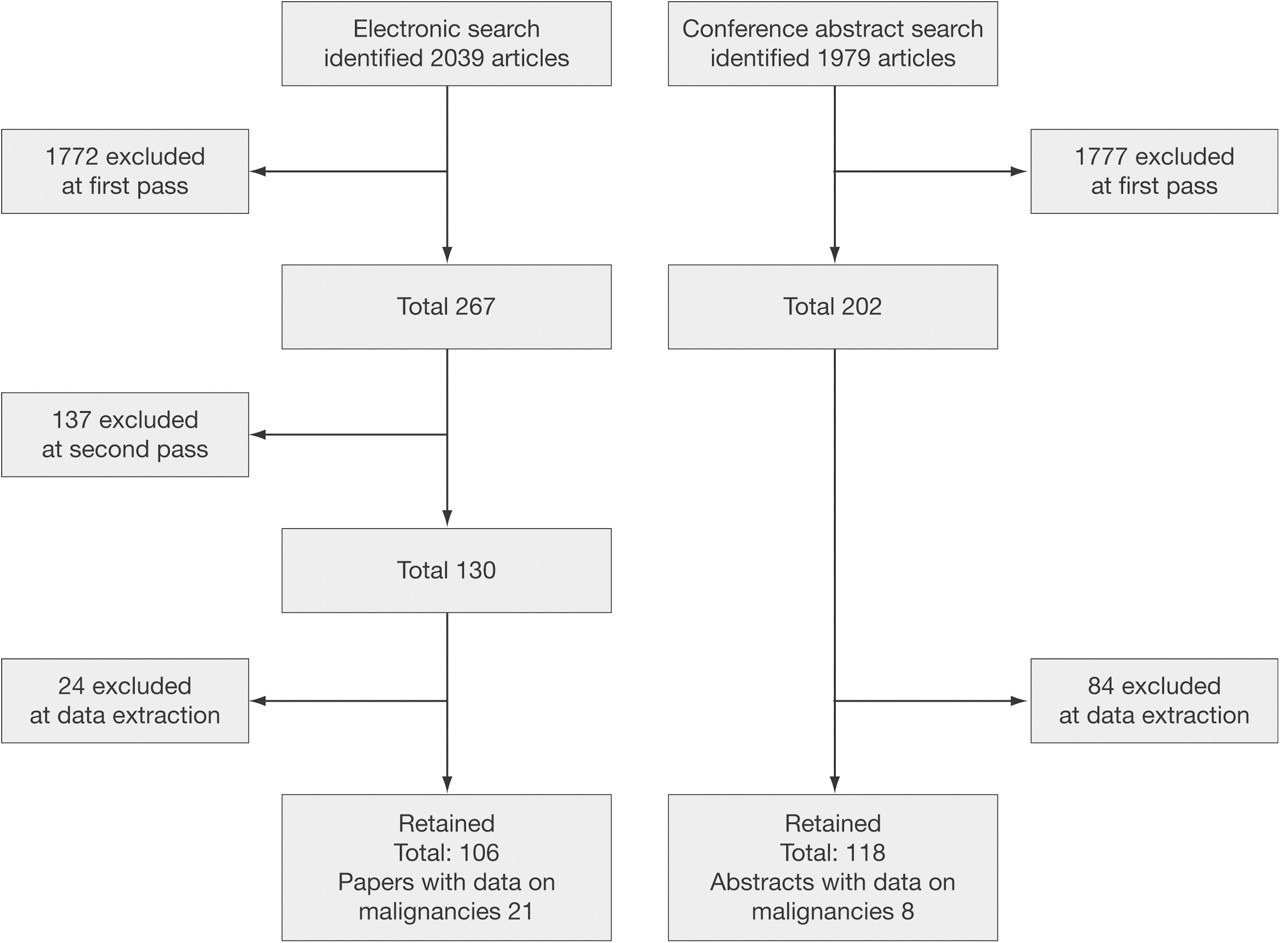
The searches identified 2039 full-text papers and 1979 conference abstracts. Figure 1 summarises the number of articles proceeding at each stage of the review and the reasons why articles were excluded. The complete list of references reviewed is available upon request from the corresponding author.

Results of review of articles identified by literature searches. Full details of the methods used for the first and second pass are provided online in the protocol. Identified articles were screened to ensure that they met the predetermined criteria. Titles and/or abstracts for all identified articles were reviewed initially at the first pass according to specific inclusion criteria (Appendix B to Full Protocol which is Appendix 1, available online only). Full-text copies of any published articles meeting the checklist inclusion criteria, plus those that could not be positively excluded, were obtained for further review. Full-text articles proceeding to the second pass were screened according to the same inclusion criteria (Appendix C to Full Protocol which is Appendix 1, available online only). The first and second pass screening results for all articles were recorded in an Excel spreadsheet.
Twenty-one full texts and eight conference abstracts reported data on malignancy associated with the use of TNFi and were therefore included.
Methodological quality
Table 1 summarises the characteristics and associated quality assessment scoring for all the included studies. Studies generally scored highly in representativeness of the exposed cohort; selection of the non-exposed cohort; ascertainment of exposure and demonstration that the outcome of interest was not present at the start of the study.
Characteristics of identified publications
Only 10 out of the 29 identified publications reported the percentage of patients lost during the follow-up period (see supplementary appendix 4, available online only). In some of the publications that did report discontinuation figures, it was not clear what proportion was actually lost to follow-up. When registry records are linked to national cancer registries (eg, ARTIS, BSRBR), it can be assumed that loss is minimal (in ARTIS it is reported as 0.3%). In other registries, the figure ranged from 6% to 19%. Malignancies were reported as part of structured questionnaires, medical records or through record linkage to cancer registries.
Analysis of malignancy rates
All-site malignancies
Rates of all-site malignancies reported in the most recent publications from each source and included in our analyses are summarised in table 2. This approach was used to avoid potential bias due to repeat inclusion of cases. In addition, data from SSATG have not been included in table 2 as these patients are included in the global Swedish national register, ARTIS. Supplementary appendices 5–7 (available online only) summarise the data from all the identified publications.
Rates of malignancies in TNFi treated patients
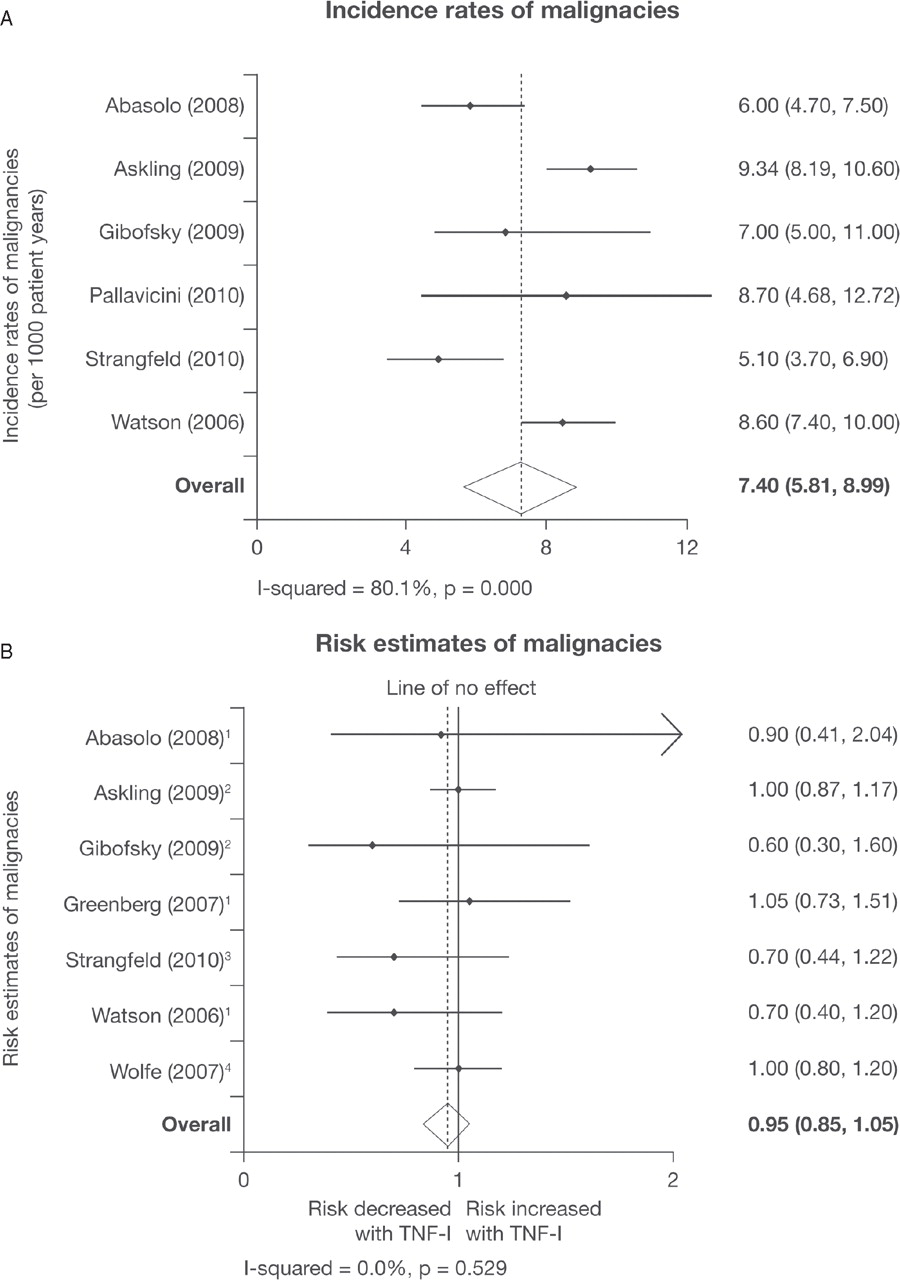
The incidence of malignancy in patients with RA ranged from 3.88 (95% CI not reported) per 1000 patient-years14 to 9.34 (95% CI 8.19 to 10.60)15 (Figure 2A). In patients with previous malignancy, rates were much higher; 25.3 (95% CI 13.4 to 43.2) per 1000 patient-years16 and 45.5 (95% CI 20.8 to 86.3) per 1000 patient-years.17

(A) Incidence rates and (B) risk estimates of malignancies reported in prospective observational studies of rheumatoid arthritis patients treated with tumour necrosis factor inhibitor (TNF-I). (B) 1, Incidence rate ratio; 2, RR; 3, HR; 4, OR.
In the most recent report from each source, RR of malignancy in TNFi-treated patients compared with RA control cohorts treated with classic disease-modifying antirheumatic drugs (DMARD) ranged from 0.6 (95% CI 0.3 to 1.6)18 to 1.05 (95% CI 0.73 to 1.51).19
For all-site malignancy, seven publications were included in the meta-analysis of RR (figure 2B). A random effects model resulted in a pooled estimate of 0.95 (0.85 to 1.05), thus indicating that treatment with TNFi was not associated with an increased risk of malignancy.
There is no evidence that longer duration of exposure to TNFi increases the risk of developing malignancy; although this was only investigated by two studies.15 20 In both cases, the RR were close to 1 over all periods examined.
Two publications have examined the risk of developing further malignancy in patients with previous malignancy before receiving treatment with TNFi. In RABBIT, the IRR for TNFi in comparison with DMARD-treated patients was 1.4 (95% CI 0.5 to 5.5, p=0.63).17 In the BSRBR, the adjusted IRR in patients with a previous malignancy was 0.58 (95% CI 0.23 to 1.43; adjusted for age and sex) and 0.45 (95% CI 0.09 to 2.17; propensity score adjusted).16 The differences between the studies may reflect the longer time from primary cancer to the start of TNFi in BSRBR compared with RABBIT (median 8.5 vs 5 years). Censoring after the first incident malignancy did not affect the results. In the analysis from RABBIT, it was reported that 14 out of the 15 cancers were true recurrences of the previous cancer,17 whereas the report from the BSRBR concluded that in most cases it was not possible to determine with any certainty whether the incident cancer was a recurrence or a new primary due to lack of sufficient clinical information.16 A random effects model was conducted and resulted in a pooled estimate of 0.62 (95% CI 0.04 to 1.20).
Specific types of malignancy
Lymphoma
Five registries reported lymphoma incidence rates, standardised incidence rates or RR.
Two reports from the NDBRD in the USA21 22 reported data in different ways. In the first publication,21 both the incidence rate (1.4 per 1000 patient-years) and SIR against the general population (2.9, 95% CI 1.7 to 4.9) were included. In the later paper,22 only an OR comparing exposed with non-exposed patients was reported (OR 1.0, 95% CI 0.6 to 1.8).
A report from a second US registry, CORRONA,19 reported a risk estimate for lymphoma of 0.74 (95% CI 0.23 to 2.45).
In ARTIS,23 the RR compared with non-exposed RA patients was 1.35 (95% CI 0.82 to 2.11) and the SIR against the general population was 2.72 (95% CI 1.82 to 4.08). A detailed analysis of data from ARTIS showed that the incidence rate was highest in patients who started treatment shortly after these agents became available. However, a longer duration of exposure or follow-up was not associated with an increased risk of lymphoma.
The regional Italian registry, LORHEN, reported SIR against the general populations of Milan and Varese of 5.99 (95% CI 1.61 to 15.35) and 4.98 (95% CI 1.34 to 12.74), respectively.24
In the French RATIO registry, cases of lymphoma associated with TNFi were identified through enhanced pharmacovigilence.25 The SIR for all patients treated with TNFi was 2.4 (95% CI 1.7 to 3.2), although there were differences between the agents with etanercept and the MAb having an SIR of 0.9 (95% CI 0.4 to 1.8) and 3.7 (95% CI 2.6 to 5.3), respectively. The other publications did not report drug-specific data19 24 or did not find any significant differences,22 23 possibly because of lack of power.
The pooled estimate from studies reporting SIR and RR was 2.55 (95% CI 1.93 to 3.17) and 1.11 (95% CI 0.70 to 1.51), respectively (figure 3). In both cases, minimal heterogeneity between the publications was present.

(A) Risk estimates and (B) standardised incidence ratios of lymphoma cases reported in prospective observational studies of rheumatoid arthritis (RA) patients treated with tumour necrosis factor inhibitor (TNF-I). (A) 1, OR; 2, RR; 3, Incidence rate ratio.
In RABBIT, one incidence of lymphoma was observed in patients treated with DMARD versus 0.9 expected from the general population, compared with five observed versus 1.9 expected in patients treated with TNFi.17 It was not reported which TNFi treatments these patients had received.
Skin cancer
Four sources reported data for skin cancer.15 19 26,–,31 In the later of the two publications from the NDBRD,31 a significantly increased risk of non-melanoma skin cancer (NMSC) in exposed patients was reported (RR 1.5, 95% CI 1.2 to 1.8, p<0.001). Non-significant increased risks for NMSC were found in CORRONA (1.83, 95% CI 0.85 to 3.93)19 and BSRBR (HR 1.7, 95% CI 0.9 to 3.4).30 The RR for squamous cell skin cancer reported from ARTIS was 1.2 (95% CI 0.8 to 2.0).28 However, the risk was apparently higher in the first year of treatment (RR 2.1, 95% CI 0.8 to 5.1).
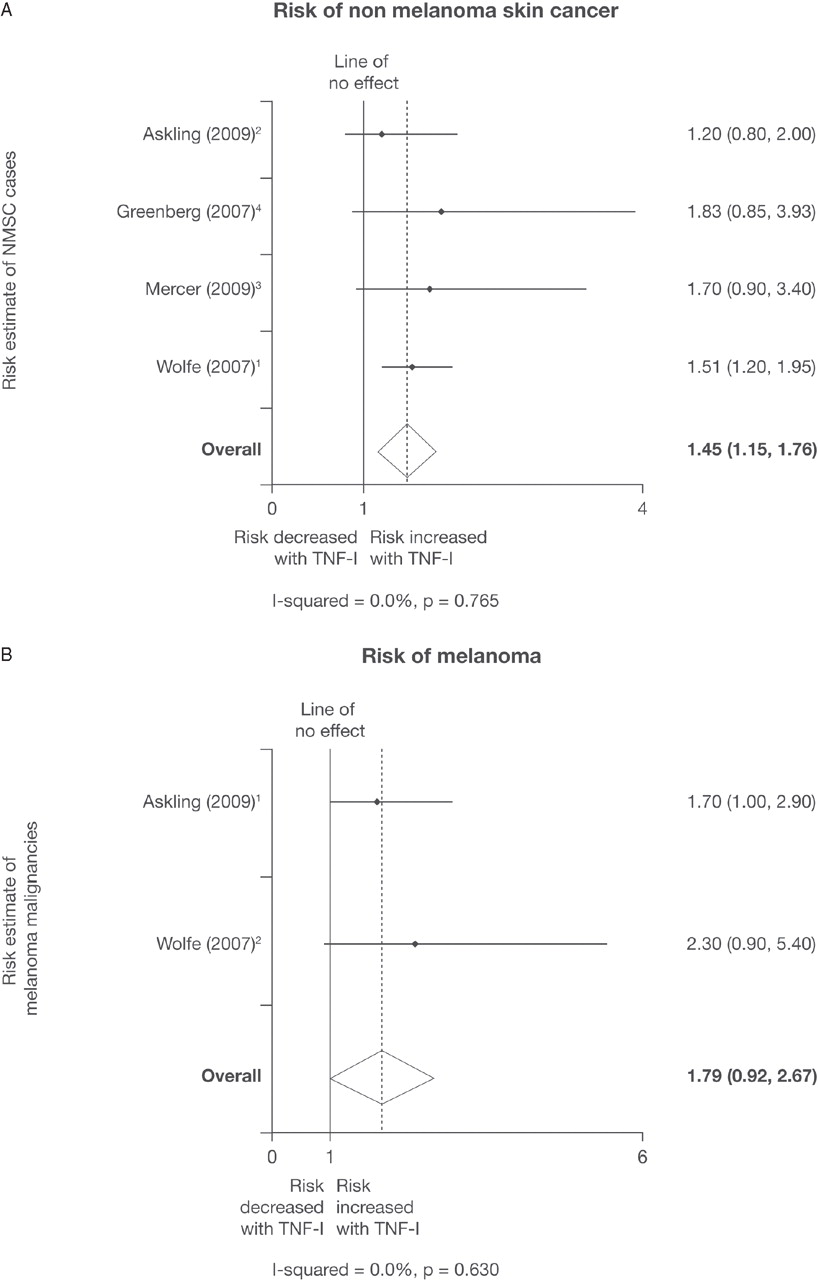
A random effects meta-analysis was carried out on the risk of NMSC compared with the TNFi-naive population (figure 4A). Patients treated with TNFi have a significantly increased risk of developing an NMSC (1.45, 95% CI 1.15 to 1.76).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk estimates of non-melanoma skin cancer (A) and melanoma (B) cases reported in prospective observational studies of rheumatoid arthritis patients treated with tumour necrosis factor inhibitor (TNF-I). (A) 1, OR; 2, RR; 3, HR; 4, Incidence rate ratio. (B) 1, RR; 2, OR. NMSC, non-melanoma skin cancer.
The NDBRD study also reported a trend towards increased risks of developing melanoma (OR 2.3, 95% CI 0.9 to 5.4)31 with similar results from ARTIS (RR 1.7, 95% CI 1.0 to 2.9).28 A pooled analysis of these data resulted in a risk of 1.79 (95% CI 0.92 to 2.67) as shown in figure 4B.
Discussion
The purpose of this systematic review was to evaluate the risks of malignancy associated with TNFi treatment, as reported in prospective registries and observational studies of biological agents and, if possible, undertake meta-analyses to provide a better estimate of the risks associated with these agents in patients treated in clinical practice. It was decided to exclude non-prospective studies and administrative databases to minimise potential heterogeneity.
In our meta-analysis of published data on all-site malignancy in general, there was no evidence that treatment with these agents increased risk when compared with non-exposed RA patients with a pooled estimate of 0.95 (95% CI 0.85 to 1.05).
In comparison with the general population, patients treated with TNFi are at an increased risk of lymphoma. However, there was no evidence that the risk of lymphoma is increased with TNFi compared with RA controls treated with classic DMARD because the point estimate was 1.11. However, the 95% CI is between 0.70 and 1.51, so a small effect cannot be excluded. This result is, however, from only three sources: ARTIS,23 NDBRD22 and CORRONA.19
It is difficult to address the question of a possible increased risk of lymphoma in RA patients treated with TNFi, because it has been demonstrated that the risk of lymphoma in RA is related to inflammatory load over time,32 and that patients treated with TNFi are those with long-term disease duration and high disease activity. Case–control studies usually adjust this parameter; however, in most cases this is cross-sectional and does not account for the change in activity over the duration of the disease. It has also been suggested that treatment with TNFi could, in some cases, reduce the risk of lymphoma by reducing activity of the disease.33
Interestingly, in the ARTIS registry, the risk of lymphoma is lower in patients treated most recently; that is patients with shorter disease duration and less severe inflammatory load, than those treated in the early 2000s.23 In spite of reassuring data from our meta-analysis, we have to be cautious because, for example, the RABBIT registry found more cases of lymphoma in patients treated with TNFi than expected in the general population (5 vs 1.9, respectively).17
This meta-analysis provides clear evidence that treatment with TNFi results in a 45% increased risk of NMSC (figure 4A). There is also an indication that the risk of melanoma is increased, although the CI were wide (0.92, 2.67) and calculated from only two studies: NDBRD31 and ARTIS28 (figure 4B).
The results of these analyses differ from a number of previous meta-analyses of RCT. Bongartz and colleagues6 7 from the Mayo Clinic published two analyses, one on the MAb infliximab and adalimumab,6 and the other on etanercept.7 The analysis of the MAb data showed an increased risk of malignancy with a pooled OR of 3.3 (95% CI 1.2 to 9.1), modified to 2.4 (95% CI 1.2 to 4.8) after the inclusion of two additional studies. However, the methodology was open to criticism, as possible differences in exposure to the interventions and comparator were not taken into account.34 Furthermore, the risk was only associated with higher doses (≥6 mg/kg infliximab over 8 weeks or ≥40 mg adalimumab every other week). The analysis of the etanercept data used individual patient information and reported an HR for malignancy compared with the control group that was raised but not significant (1.84, 95% CI 0.79 to 4.28). In contrast with these meta-analyses, others have found no increased risk of malignancy, although published 95% CI include clinically meaningful increased risks (RR 1.5, 95% CI 0.8 to 3.0 (all-site malignancy); OR 1.26, 95% CI 0.52 to 3.06 (lymphoma); OR 1.27, 95% CI 0.67 to 2.42 (NMSC)).35 36
Remarkably similar results to those reported in this review were found in a recently published meta-analysis of RCT.37 The analysis included studies of 15 418 patients treated with TNFi and 7486 patients treated with DMARD. The results showed that TNFi treatment was not associated with an increased risk of all-site malignancy (RR 0.99, 95% CI 0.61 to 1.68), apart from NMSC in which the risk was increased (RR 2.02, 95% CI 1.11 to 3.95).
In further support of our meta-analysis results, data obtained from pooling two US and one Canadian administrative database showed no significantly increased risk of either solid (HR 0.91, 95% CI 0.65 to 1.26) or haematological malignancies (HR 1.37, 95% CI 0.71 to 2.65).38 These results are very similar to those reported in our publication.
Meta-analyses of observational studies must be considered with caution. Potential issues include publication bias, inappropriately combining different measurements of risk (risk difference, OR, HR, RR) and pooling studies when there is significant heterogeneity (study level and/or patient level). Analyses of observational studies are particularly challenging because of study design and inherent biases due to non-randomisation. In order to minimise these issues, we used appropriate methods to address these potential pitfalls.
It is known that the indexing of observational studies is sometimes problematical.39 However, every attempt was made to ensure that all potential references were identified, both by changes to the search criteria and hand searching of reference lists.
The included studies involved more than 40 000 patients and almost 150 000 patient-years of exposure. This large dataset overcomes the issues regarding limited numbers in the RCT. Furthermore, to some extent, the longer exposure times overcomes the issue regarding the short duration of the trials. However, given the long latency associated with many cancers, follow-up should be extended even further to assess whether TNF inhibition increases the risk of malignancy.
The issue of potential bias also needs to be considered when evaluating data from observational studies.40 Potential biases include selection and surveillance bias, selection of the reference cohort, confounding by disease severity, channelling bias and depletion of the more susceptible patients. In light of the known involvement of TNF in cancer surveillance, patients initiating treatment with inhibitors of this cytokine will be carefully evaluated and those at potential cancer risk not prescribed these agents. This approach could potentially result in an apparently lower risk in the exposed patients such that RR are reduced. This effect may explain the higher risks reported in the Mayo Clinic analyses6 7 than in this report. It is thus interesting to focus on patients with previous malignancy treated with a TNFi because such bias may be reduced in these patients.
While it may be recommended that patients with previous malignancy should not be treated with TNFi, data from two separate sources show no significantly increased risk compared with DMARD-treated patients with previous malignancy, although the upper 95% CI include clinically meaningful increased risks (1.4316 and 2.1717). This does not mean, however, that this practice may be relaxed, rather that in those patients who were selected for treatment with TNFi, there was no increased risk of recurrence or a new primary cancer. Therefore, the current approach of physicians to such patients is appropriate. Patients treated with TNFi may also be seen more often and evaluated with greater suspicion when symptoms suggestive of malignancy are reported so that cases are detected earlier than in the reference cohorts, a form of surveillance bias that would lead to an apparent increased risk of malignancy in the exposed groups. This could be particularly true for NMSC.
Although the overall data are reassuring, the results must be considered with caution due to the limited duration of follow-up and potential biases discussed above. In addition, only very limited data are available for site-specific cancers with the exception of skin cancers, and so do not allow any conclusions to be drawn. Moreover, very few data are available for patients with other rheumatic diseases.
This systematic review and meta-analysis provides reassurance to physicians and patients that the treatment of RA patients with TNFi does not increase the risk of malignancy, particularly lymphoma. However, it does appear to increase the risk of skin cancer, including melanoma. The CI, however, do not preclude an effect of treatment on the risk for specific malignancies, and researchers should be encouraged to publish additional analyses to add to the evidence base.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
-
Funding The literature searches and data extraction were funded by a grant from Wyeth Europa (Wyeth was acquired by Pfizer in October 2009) to the Evidence Research Unit. Wyeth Europa paid author travel and accommodation costs to attend meetings at which this systematic review was discussed. None of the authors received payment for their contributions to this manuscript.
-
Competing interests XM has received honoraria for talks or participation in advisory boards from Roche, UCB, Wyeth (acquired by Pfizer in October 2009). MM-C has received fees for lectures from Wyeth, Pfizer, Actelion, BMS, Roche and research grants from Pfizer, Actelion, Schering-Plough, Centocor. KP has received fees as a consultant to Abbott, Schering-Plough, Roche and Wyeth. PT has received research grants from Merck, UCB, AstraZeneca, GlaxoSmithKline and Roche. He has been an invited speaker and advisor for Abbott, Bristol-Myers Squibb, Centocor, Roche, Schering-Plough, Wyeth and UCB. RvV has received research support and honoraria from Abbott, Bristol. Myers Squibb, Roche, Schering-Plough, UCB Pharma and Wyeth. RH was supported by a grant from Wyeth Europa. CW was supported by a grant from Wyeth Europa. RL was supported by a grant from Wyeth Europa. AR was an employee of Wyeth Europa and had held shares in Wyeth and currently has Pfizer share options. Work undertaken since leaving the company in June 2010 has been funded by Pfizer. PE has received research grants and honoraria from Abbott, Bristol. Myers Squibb, Roche, MSD, UCB Pharma and Wyeth.
-
Provenance and peer review Not commissioned; externally peer reviewed.