Article Text

Abstract
Background Cardiovascular (CV) disease has a major impact on patients with rheumatoid arthritis (RA), however, the relative contributions of traditional CV risk factors and markers of RA severity are unclear. The authors examined the relative importance of traditional CV risk factors and RA markers in predicting CV events.
Methods A prospective longitudinal cohort study was conducted in the setting of the CORRONA registry in the USA. Baseline data from subjects with RA enrolled in the CORRONA registry were examined to determine predictors of CV outcomes, including myocardial infarction, stroke or transient ischemic attack. Possible predictors were of two types: traditional CV risk factors and markers of RA severity. The discriminatory value of these variables was assessed by calculating the area under the receiver operating characteristic curve (c-statistic) in logistic regression. The authors then assessed the incidence rate for CV events among subjects with an increasing number of traditional CV risk factors and/or RA severity markers.
Results The cohort consisted of 10 156 patients with RA followed for a median of 22 months. The authors observed 76 primary CV events during follow-up for a composite event rate of 3.98 (95% CI 3.08 to 4.88) per 1000 patient-years. The c-statistic improved from 0.57 for models with only CV risk factors to 0.67 for models with CV risk factors plus age and gender. The c-statistic improved further to 0.71 when markers of RA severity were also added. The incidence rate for CV events was 0 (95% CI 0 to 5.98) for persons without any CV risk factors or markers of RA severity, while in the group with two or more CV risk factors and three or more markers of RA severity the incidence was 7.47 (95% CI 4.21 to 10.73) per 1000 person-years.
Conclusions Traditional CV risk factors and markers of RA severity both contribute to models predicting CV events. Increasing numbers of both types of factors are associated with greater risk.
Statistics from Altmetric.com
Introduction
Cardiovascular (CV) disease represents a major source of morbidity and mortality for patients with rheumatoid arthritis (RA).1,–,4 Myocardial infarction (MI) and stroke are common events and thus difficult for a single clinician to associate with a given disease, such as RA. However, a series of large epidemiologic studies over the last several decades strongly support an elevation in CV risk with RA.3 4 These studies have come from both community-based and referral populations, and consistently find that RA patients have a 1.5 to 3-fold increased risk for CV events compared with non-RA controls. In addition to the increased risk of CV events in RA, silent cardiac ischemia and fatal CV presentations may be more common in RA than in non-RA subjects.5,–,7
In spite of the clear association between CV events and RA, elucidating the link between these conditions has been challenging. Some, but not all, studies suggest that the heightened CV risk is mediated by an effect of RA on traditional CV risk factors, such as hyperlipidemia and insulin resistance.8,–,10 Other data demonstrate that markers of RA severity associate with surrogate markers of CV risk; for example, elevated acute phase reactants correlate with an increased carotid intima medial thickness.11 In patients with new onset inflammatory polyarthritis, C-reactive protein (CRP) levels are directly related to risk of death.12 Other results have also supported the relationship between RA disease activity and CV risk.13 There are also data suggesting an association between rheumatoid factor (RF) and CV events.14 Some medications used for RA have been linked with CV risk – glucocorticoids and non-steroidal anti-inflammatory drugs. However, these agents do not appear to completely explain the CV risk associated with RA.13 15 16
Several prior studies have demonstrated an association between CV risk factors, markers of RA severity and atherosclerosis.17 18 These studies have been consistent in their findings, but none have used actual CV events as an outcome.
A more complete understanding of risk factors for CV events in RA will facilitate development and testing of intervention strategies. On a population level, better control of traditional CV risk factors will likely lead to fewer CV events in RA, but it is unclear whether a strategy of enhanced control of RA disease activity will also lead to reduced CV risk. Moreover, there is no information on the relative importance of targeting traditional CV risk factors versus markers of RA severity to affect CV risk. We thus examined the relative importance of baseline traditional CV risk factors compared with baseline markers of RA severity to determine their relative predictive value for CV events in a very large longitudinal cohort. This work was guided by the hypothesis that both sets of factors would add independent predictive value to models of CV events among patients with RA.
Methods
Study cohort
We examined data from CORRONA, the Consortium of Rheumatology Researchers of North America. Since 2002, CORRONA has enrolled over 17 000 patients with RA through 268 participating academic and community rheumatologists at 103 sites in the USA. Rheumatologists and their staff receive training on patient recruitment and form completion. They are reimbursed for the collection of data at the time of the routine clinical encounter on consecutive patients in a prospective manner. For the purposes of the current analyses, we included only patients diagnosed with RA and not Psoriatic Arthritis, who contributed information to CORRONA on at least three rheumatology visits. All patients satisfied the ACR criteria according to the enrolling Rheumatologist. No specific selection criteria are applied to enrolling patients with RA. Follow-up began with the baseline CORRONA visit and continued through December 31, 2006, an endpoint or loss to follow-up, whichever came first.
All subjects have given written informed consent and the study protocol has been approved by the appropriate Institutional Review Board.
Endpoints
The CV events considered in this analysis include major ischemic events, but not heart failure or peripheral arterial disease. The rationale for this decision is that other predictive models of CV events, such as the Framingham Risk Score, were developed to predict ischemic CV events.19 In addition, while ischemia is an important factor in heart failure, the risk factors can be different. We examined follow-up rheumatologist assessment forms for reports of new CV events, including MI, stroke or transient ischemic attack (TIA). There were specific questions for each of these endpoints on the forms for the study period (2002–2006), but not for unstable angina. In addition, because death certificates were not available for the majority of patients, we chose to exclude CV-related deaths for this study. These reports prompted a follow-up inquiry to the rheumatologist to confirm the report, determine if it was a new event and the date of the event. Medical records were then requested regarding the event.
To test the validity of the rheumatologist-confirmed CV events, a three-person Adjudication Committee comprised of two board-certified cardiologists and an internal medicine specialists reviewed the 56% (42 of 75) of cases of MI, stroke and TIA reported by participating rheumatologists for which hospitalization records where available. All events were classified into one of four possible categories: definite, probable, possible and unlikely CV events. Events adjudicated as definite (31%) or probable (65%) events were considered as true events for the purposes of validation (see Supplemental file for further explanation of the adjudication criteria). Case definition criteria for MI, stroke and TIA were applied by the adjudication committee as previously defined. The MI adjudication criteria were consistent with definitions from the American Heart Association guidelines for both ST segment elevation and non-ST-segment elevation MI. The stroke case definition was consistent with the American Heart Association/American Stroke Association guidelines.20 (See Supplemental file for details of adjudication criteria.) The positive predictive value for confirmed cases where records were available was 96%. (See Supplemental file for details of confirmation process.)
The primary analysis used all CV events confirmed by rheumatologists. Sensitivity analyses used definite or probable events based on the adjudication committee review.
Potential predictors
Both patients and their rheumatologists complete assessment forms at all visits, typically occurring every 3–6 months (mean 4.5 months). Age was defined at the time of enrolment. The baseline forms focus on RA disease characteristics, functional status, disease activity and medication use, as well as family history of diseases, including CV disease. Acute phase reactants (CRP or ESR) were not available in all subjects and thus were not considered in these analyses. We combined data regarding autoantibody status – RF and antiCCP antibody – into a composite ‘seropositive’ variable. Seven variables were available in most patients and considered as potential markers of RA severity: longer disease duration (>5 years),3 the presence of radiographic joint erosions, the presence of subcutaneous nodules, prior total joint replacement, modified Health Assessment Questionnaire score ≥2,21 a Clinical Disease Activity Index (CDAI) score >22,22 and seropositivity. The CDAI combines swollen and tender joint counts, a physician's assessment of global arthritis activity and a patient's assessment of arthritis activity, but does not require an inflammatory marker.
Traditional CV risk factors were also collected from the baseline rheumatologist and patient questionnaire. These included six variables – hypertension, diabetes, treated hyperlipidemia, current tobacco use, known CV disease (such as prior MI) and a family history of premature CV events (at age <50 years). The hyperlipidemia variable was based on the use of a lipid-lowering agent. No information was available on subject's actual blood pressure or lipid levels. Known CV disease was based on a report of prior MI, stroke, TIA or coronary intervention, such as stenting or a coronary artery bypass graft.
Statistical analysis
The patient cohort was described according to their RA and CV characteristics. Since our goal was to examine the predictive accuracy of groups of variables measured at baseline, that is, traditional CV risk factors and markers of RA severity and not a given variable, we did not use the univariate parameter estimates to determine which variables to place in the multivariable models. The potential markers of RA severity were chosen a priori and based on variables without substantial missing data. This tends to lead to a less overfit model.
We assessed the accuracy of these variables using several different model fit statistics, evaluating both the discrimination and calibration of the various models. Discrimination refers to the ability of a model to accurately predict which subjects experience an endpoint. The area under the receiver operating characteristic curve, measured as the c-statistic, is a commonly used measure of model discrimination that can be obtained from the logistic model.23 The c-statistic is considered a measure of how well a model with one or several variables can discriminate between one outcome and another, with a c-statistic of 0.50 being no better than chance and 1.0 being perfect. Calibration describes a model's ability to determine levels of risk. The Akaike Information Criterion (AIC), a goodness of fit test, was assessed from the logistic regression models.24 The AIC allows one to compare a given model's predicted values with actual values.
Finally, the incidence rate of CV events and 95% CI were calculated for subjects with different numbers of each type of risk factor. For this analysis, age ≥75 years and male gender were considered traditional CV risk factors. Thus, there were eight potential traditional CV risk factors and seven markers of RA severity. By examining the incidence rate in this stratified analysis, we are able to adjust for these confounders without making any assumptions about the covariate matrix. All analyses were run using SAS Statistical Software (version 9.0, Cary, North Carolina).
Results
The study cohort included 10 156 subjects followed for a median of 22 months. At cohort entry, the subjects had a mean age of 59 years and 75% were female. The median disease duration at the start of follow-up was 84 months and 72% were seropositive. The median modified HAQ was 0.8 with rheumatoid nodules noted among 20.1% and total joint replacement among 30.4%. Traditional CV risk factors are also listed in table 1. Diabetes was present in 7.1% of subjects, hypertension in 29.8%, hyperlipidemia in 9.2% and current tobacco use in 16.1%. Family history of premature CV events was noted by 5.1% of subjects. As well, 8.5% of subjects reported prior CAD as evidenced by an MI, stroke, TIA, angina or coronary intervention. Baseline use of treatments for RA included: 63% methotrexate, 35% tumour necrosis factor (TNF) blocker and 17% other DMARDs.
Baseline characteristics of study population with rheumatoid arthritis in CORRONA (n=10 156)
During the 18 829 patient-years of follow-up, 29 MIs and 47 strokes or TIAs were reported and confirmed by rheumatologists. As shown in table 2, the event rates was 3.98 (95% CI 3.08 to 4.88) per 1000 person-years. The event rates were higher for patients 75 years and over versus those younger than 75 years and for men versus women (see table 2).
Cardiovascular event rates by age and gender among CORRONA subjects with rheumatoid arthritis
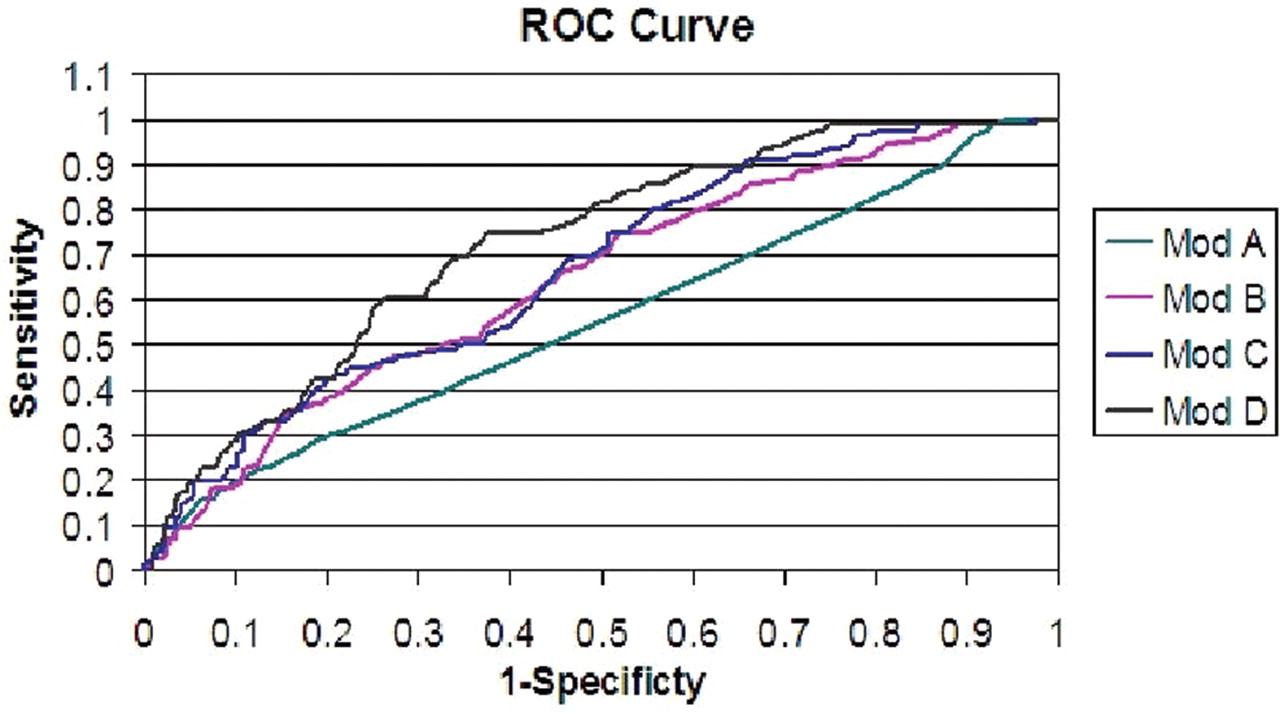
Several logistic models were fit – traditional CV related factors only (Model A), markers of RA severity (Model B), both types of variables (Model C), both types of variables plus age and gender (Model D). The goal of these models was not to determine the risk associated with an individual factor, but rather to compare the models' characteristics. The area under the receiver operating characteristic curves improved with each subsequent model: Model A c-statistics=0.57, Model B c-statistic=0.64, Model C c-statistic=0.66 and Model D c-statistic=0.71 (see figure 1). In an alternative analysis, the c-statistic improved from 0.67 to 0.71 (p=0.0061) when markers of RA severity were added to the traditional CV risk factors plus age and gender. The increase in c-statistic was larger when RA severity measures were added to age and gender (change in c-statistic=0.07) than when the CV risk factors were added (change in c-statistic=0.04). As well, the AIC improves (lower values) incrementally across the models types of variables are added: Model A AIC=898, Model B AIC=895, Model C AIC=897, Model D AIC 887. (Each model's AIC and c-statistic were calculated using the same cohort to avoid sample size impacting AIC). The sensitivity analysis using only definite or probably CV events according to the adjudication committee yielded similar results (see Supplemental file).

{kind=link}
The Figure illustrates the area under the receiver operating characteristic curves for four multivariable logistic models predicting cardiovascular events among subjects with rheumatoid arthritis: Model A contains only traditional cardiovascular risk factors (c-statistic 0.57), Model B contains only markers of RA severity (c-statistic 0.64), Model C contains both types of factors (c-statistic 0.66) and Model D adds age and gender to Model C variables (c-statistic 0.71).
Finally, we calculated the number of traditional CV risk factors and RA markers (see table 3) and then the incidence rates for CV events based on the number of factors (see table 4). While the increase in risk was not continuous across all categories of risk factors because of few events, there was a clear trend toward an increased risk with more traditional CV risk factors and markers of RA severity. Subjects without any risk factors or markers of RA severity had an incidence rate of 0 (95% CI 0 to 5.98) CV events per 1000 person-years, while subjects with two or more traditional CV risk factors and three or more markers of RA severity had an incidence rate of 7.47 (95% CI 4.21 to 10.73) per 1000 person-years.
Cardiovascular events among subjects in CORRONA with different numbers of traditional cardiovascular risk factors and markers of rheumatoid arthritis severity
The incidence rate (95% CI) of cardiovascular events by various combinations of traditional cardiovascular risk factors and markers of rheumatoid arthritis severity
Discussion
CV disease is a major co-morbidity for patients with RA. However, relatively little information is available to determine which RA patients are at risk of CV events and the relative contributions of traditional CV risk factors versus markers of RA severity. We examined these issues using the CORRONA registry, a very large prospective RA cohort from the USA. Both traditional CV risk factors and markers of RA severity contributed independent information to predict risk of future CV events. When both types of variables were included, the model's discrimination improved. Markers of RA severity added to the model's c-statistic above and beyond the traditional CV risk factors plus age and gender. Moreover, with increasing numbers of either type of variable, there was a trend toward increasing incidence rates of CV events.
Our data support the important independent contributions of both traditional CV risk factors and markers of RA severity to CV risk models. In models with both types of variables plus age and gender, we observed a c-statistic comparable to those calculated for analyses of the Framingham Risk Score.25 Our findings largely confirm prior work that focused on surrogate CV endpoints.17 18 While epidemiologic data do not substitute for treatment trials, these results suggest that strategies to reduce CV risk should focus on a strategy of controlling both traditional CV risk factors as well as controlling RA severity. In addition, it would be interesting to tailor interventions based on the risk factor profile. For example, patients with a greater number of markers of RA severity might be targeted for more intensive control of traditional CV risk factors, such as LDL lowering with statins, as well as better control of their RA disease activity.
There currently are no CV treatment trial data specific to RA patients. There are data from non-RA patients supporting the benefits of HMG CoA reductase inhibitors (‘statins’) for secondary prevention and primary prevention in high risk groups.26 In addition, the trial of atorvastatin in rheumatoid arthritis (TARA) trial found that statins effectively lower lipid levels in patients with RA and resulted in small decrements in CRP, while also modestly reducing disease activity.27 One large trial of statins for primary prevention of CV disease events in patients with RA is ongoing, however no results are expected until at least 2011.28 Interestingly, a recently published trial of statin use in persons without hyperlipidemia but an elevated CRP found a significant reduction in CV events in the statin arm.29 The authors hypothesise that an independent anti-inflammatory effect of high-dose statin therapy could contribute to a diminished CV risk. If this is the case, it follows that other RA interventions which substantially reduce inflammation might also result in similar effects. Several observational studies found reduced CVD morbidity and mortality among methotrexate users.30 31 In addition, TNF antagonists may improve endothelial function.32 However, studies with actual CV endpoints demonstrate mixed findings.13 15 33
The strengths of the current study are the large number of subjects with RA, the inclusion of traditional CV risk factors and markers of RA severity derived from both rheumatologists and patients and the use of confirmed and adjudicated CV events. However, several limitations are important to discuss. First, while the CORRONA cohort is large, there were relatively few CV events included in this analysis, resulting in few events in certain cells in table 4. The majority of endpoints included were confirmed by the treating rheumatologist, and the majority was adjudicated by a panel of cardiologists based on primary data. Medical records could not be obtained for some of the confirmed endpoints. These hospital medical records are not routinely received by USA rheumatologists when patients are hospitalised, and CORRONA does not have patient personal identifiers or patient consent to directly request these records. Thus, the investigator needs to obtain the records for CORRONA. Because some hospital records were requested for events occurring as remotely as 2002, records were not obtained on all patients. It would have been ideal to include coronary re-vascularisation, but this information was not included in the CORRONA assessment forms used at the time these data were collected. Second, it is possible that there is some under-ascertainment of CV events. Fewer composite events may have been observed because the data collection forms for the study period (2002–2006) did not have information on unstable angina. In addition, because death certificates were not available for the majority of patients, we chose to exclude CV-related deaths for this study. However, based on reference populations such as the WHO MONICA Study, one might have anticipated 1.34 events per 1000 person-years.34 We found 3.98 events per 1000 person-years in this cohort with RA, a group with a relative risk of CV events of 1.5 to 3.0. Thus, we believe that under-ascertainment was not a major problem. It is also possible that the higher utilization rate for biologic DMARDs could have influenced the rate of CV events which we observed. Because of the large percentage of these patients who utilised biologic DMARDs or MTX, it is also possible that the incidence of CV events in this population would be lower than that described in European populations in which a much smaller percentage of patients with RA receive these agents.35 As has recently been described, diverse sources of epidemiologic information derived from different societies serve to enhance insights.36 Third, detailed data on actual blood pressure and lipid measurements were not collected and thus it is possible that hypertension and hyperlipidemia were under-reported. Literature estimates of hypertension and hyperlipidemia in similar cohorts argues against under-reporting.37 38 This limitation has been addressed in current versions of CORRONA forms. Finally, data on acute phase reactants are not mandated in CORRONA and therefore these data were incomplete. However, the CDAI (which does not require an acute phase reactant) is highly correlated with the Disease Activity Score (which does include an acute phase reactant).39
In conclusion, we found that both traditional CV risk factors and markers of RA severity were important predictors of future CV events in this very large US cohort. The risk added by RA-related factors added independent information to the predictive models. However, our models only explain a portion of the variability, likely because of imprecision in variable measurement as well as there being other variables not included in our adjusted models. These might include serologic markers, medications and genetics. The European League Against Rheumatism has recently published recommendations for CV risk management among patients with RA.40 These recommendations acknowledge the importance of both traditional CV risk factors and RA-specific variables, similar to our analyses. The proportion of variation explained by both types of factors is similar, suggesting that both traditional CV risk factors and markers of RA disease severity can be appropriately targeted to lessen the incidence of CV events, the major source of mortality in patients with RA.
Acknowledgments
The Adjudication Committee included Dr Michael Farkouh, Dr Simonette Sawit and Dr Sameer Bansilal.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Support: There was no specific support for these analyses. CORRONA has received general support in the last two years from Abbott, Amgen, BMS, Centocor, Genentech, Lilly and Roche. Dr. Solomon receives salary support from research grants from the NIH (AR AR055989 and AR 047782), AHRQ, the Arthritis Foundation, Abbott and Amgen. Jeffrey Curtis receives salary support from NIH (AR053351). Dr. Farkouh receives salary support from the NIH (HL071988 and HL092989). Dr Greenberg receives salary support from the NIH (K23AR054412) and the Arthritis Foundation.
-
Funding Other Funders: Abbott, Amgen, BMS, Centocor, Genentech, Lilly and Roche.
-
Competing interest CORRONA has received general support in the last two years from Abbott, Amgen, BMS, Centocor, Genentech, Lilly and Roche. Dr. Solomon receives salary support from research grants from the NIH (AR AR055989 and AR 047782), AHRQ, the Arthritis Foundation, Abbott and Amgen. Jeffrey Curtis receives salary support from NIH (AR053351). Dr Greenberg receives salary support from the NIH (K23AR054412) and the Arthritis Foundation.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Ethics approval This study was conducted with the approval of the CORRONA.