Article Text

Abstract
Objectives: To compare receptor activator of NF-κB ligand (RANKL) production in the synovial tissue from patients with active rheumatoid arthritis (RA), inactive RA, spondyloarthropathies (SpA), osteoarthritis, and from normal subjects. In addition, to establish the cell lineages expressing RANKL in these tissues.
Methods: Immunohistological analysis of frozen synovial tissue biopsy specimens was performed using a monoclonal antibody (mAb) to detect RANKL. Sections were evaluated by computer assisted image analysis and semiquantitative analysis to compare RANKL expression between groups. Dual and sequential labelling with mAb RANKL and cell lineage specific monoclonal antibodies were used to determine the types of cells expressing RANKL.
Results: Higher levels of RANKL were expressed in tissues from patients with active RA and SpA than in tissues from patients with inactive RA, osteoarthritis, and from normal subjects. RANKL protein was associated with CD3 antigen-positive lymphocytes and some macrophages. RANKL was predominantly associated with activated, memory T cells (CD45Ro positive cells) in patients with active RA and spondyloarthropathy (SpA).
Conclusions: The highest levels of RANKL were detected in patients with RA with active synovitis and in some patients with SpA. An increase in RANKL in the inflamed joint of patients with RA, produced by infiltrating activated T cells and macrophages, is likely to be an important cause of joint erosions in RA.
- bone
- rheumatoid arthritis
- receptor activator NF-κB ligand
- immunohistochemistry
- spondyloarthropathies
- AEC, 3-amino-9-ethylcarbazole
- DIA, digital image analysis
- FLS, fibroblast-like synoviocytes
- HRP, horseradish peroxidase
- IL, interleukin
- IOD, integrated optical density
- mAb, monoclonal antibody
- MOD, mean optical density
- OA, osteoarthritis
- OPG, osteoprotegerin
- RA, rheumatoid arthritis
- RANK, receptor activator of NF-κB
- RANKL, receptor activator of NF-κB ligand
- SpA, spondyloarthropathy
- SQA, semiquantitative assessment
- TNF, tumour necrosis factor
Statistics from Altmetric.com
- AEC, 3-amino-9-ethylcarbazole
- DIA, digital image analysis
- FLS, fibroblast-like synoviocytes
- HRP, horseradish peroxidase
- IL, interleukin
- IOD, integrated optical density
- mAb, monoclonal antibody
- MOD, mean optical density
- OA, osteoarthritis
- OPG, osteoprotegerin
- RA, rheumatoid arthritis
- RANK, receptor activator of NF-κB
- RANKL, receptor activator of NF-κB ligand
- SpA, spondyloarthropathy
- SQA, semiquantitative assessment
- TNF, tumour necrosis factor
Rheumatoid arthritis (RA) is a chronic inflammatory disease characterised by articular cartilage and bone destruction following growth of the inflamed synovial tissue over the articular surface. Extensive bone erosion is often seen as marginal joint erosions radiographically, and is predictive of a poorer prognosis.1 This inflammation and tissue destruction in RA is thought to involve cell-cell interactions between lymphocytes, monocytes/macrophages, and type A and B synoviocytes. These cell interactions result in the production of matrix metalloproteinases, cathepsins, and mast cell proteinases that cause cartilage and bone destruction.2–4 Osteoclast formation from cells of the macrophage/monocyte lineage at the cartilage-pannus junction is associated with the destruction of bone matrix in patients with RA.5–8
A number of inflammatory cytokines found in the RA synovial fluid and tissue (interleukin (IL)1α and β, IL6, tumour necrosis factor (TNF)α, macrophage colony stimulating factor) have the potential to promote osteoclast formation and bone resorption.9–13 These may act by increasing production of the receptor activator of NF-κB ligand (RANKL), a recently identified primary mediator of osteoclastogenesis.14 RANKL and its receptor, RANK (receptor activator of NF-κB), are key factors in osteoclast formation5,6,15 and regulation of the immune system.16 RANKL is expressed by osteoblasts/stromal cells,15 fibroblasts,5,6,17 and activated T cells5,18,19 and binds directly to RANK on pre-osteoclasts and osteoclasts, enabling signal transduction for the differentiation of osteoclast progenitors as well as activation of mature osteoclasts.15,20,21 In addition to their pivotal role in osteoclast formation, RANKL and RANK have a role in immune cell differentiation and T cell/dendritic cell interactions.16,22–24
Osteoprotegerin (OPG), a soluble TNF receptor-like molecule, is the naturally occurring inhibitor of RANKL. OPG acts as a decoy soluble receptor preventing osteoclastogenesis by binding to RANKL with high affinity, essentially blocking RANKL from interacting with RANK both in vivo and in vitro.20,25,26 The fundamental role of these molecules in regulating bone morphology has been clearly demonstrated in transgenic and knockout mice.16,25,27,28
We have reported mRNA expression of RANKL, RANK, and OPG in cells isolated from RA joints and the significant correlation between the number of resorption pits formed by cells extracted from these tissues and the ratio of RANKL mRNA to OPG mRNA.8 More recently, we found that the level of OPG protein, detected in situ by immunohistochemistry, is markedly decreased in patients with RA with active synovitis compared with patients with inactive RA, osteoarthritis (OA), and normal subjects.29 This study compared the protein expression of RANKL in the synovial tissue from patients with active RA with that seen in patients with inactive RA, spondyloarthropathies, OA, and in normal subjects. A unique aspect of this study is the use of semiquantitative and quantitative techniques to measure synovial tissue staining of RANKL protein in patients with a range of inflammatory and non-inflammatory arthritides. Using this data, we aimed at testing the hypothesis that RANKL protein is expressed at higher levels in patients with RA with active disease than in synovial tissue from patients with inactive RA or other arthritides.
In addition, we used dual immunohistochemical labelling techniques and sequential staining to verify the cell lineages expressing RANKL in these tissues. This enabled us to investigate the controversial role of T cells and macrophages in the localised bone loss associated with RA.
PATIENTS AND METHODS
Patients
Thirty patients with RA (21 with active synovitis in a knee joint and nine with no evidence of any synovitis) and 12 patients with a spondyloarthropathy (SpA) and active synovitis of a knee joint were investigated together with seven patients with OA of the knee joint and 18 normal subjects. All patients with RA fulfilled the American College of Rheumatology criteria for RA,30 while the patients with SpA fulfilled the European Spondylarthropathy Study Group (ESSG) criteria for the diagnosis of ankylosing spondylitis and Reiter's disease.31 Patients with psoriatic arthritis32 and OA of the knee33 fulfilled published criteria. Table 1 summarises details of the patients and drugs used at the time of surgery. The study protocol was approved by the institutional medical ethics committee under the condition that the patients included gave their informed consent.
Demographic and clinical details of the patients with RA and SpA included in the study
Synovial tissue
A small-bore arthroscopy (2.7 mm arthroscope; Dyonics, Andover, Massachusetts, USA) was performed under local anaesthesia as previously described.34 Biopsy specimens of synovial tissue from patients with RA were obtained from all accessible regions of the knee joint, but mainly from the suprapatellar pouch. OA synovial tissue was obtained at the time of knee replacement surgery and normal synovial tissue was obtained at the time of knee arthroscopy for unexplained knee pain. The samples were separately snap frozen in Tissue-Tek OCT (Miles Diagnostics, Elkhart, IN, USA) and stored at −80°C until used. Sections (5 μm) were cut on a cryostat and mounted on APTS (Sigma, St Louis, MO, USA) coated glass slides. The glass slides were boxed and stored at −20°C until immunohistological analysis.
Immunohistochemistry
Serial sections were stained with the following mouse monoclonal antibodies (mAb): antihuman RANKL antibody (MAB626; R&D Systems, Inc, Minneapolis, MN, USA) and anti-CD68 (EBM11; DAKO) to detect macrophages; mAb 67 (Serotec, Kidlington, Oxford, UK), which recognises CD55, to detect fibroblast-like synoviocytes (FLS); anti-CD22 (CLB) to detect B cells; anti-CD3 (Becton Dickinson, CA, USA) to detect pan-T cells; and anti-CD45Ro (UCHL1; DAKO, Denmark) for activated, memory T cells. To eliminate variability in immunohistochemical staining, all sections to be stained with a particular antibody were processed in the same run and the antibody was left on for the same amount of time. The absence of staining was identical to that obtained when a non-specific primary antibody was used.35 In addition, blocking the activity of the RANKL antibody by preincubation for 24 hours with excess human recombinant RANKL (a gift from AMGEN Inc, Thousand Oaks, CA, USA) nearly eliminated staining (data not shown).
Endogenous peroxidase activity was inhibited by 0.1% sodium azide and 1% hydrogen peroxide in Tris/phosphate buffered saline buffer. After incubation with the primary mAb RANKL 626 (or CD45Ro in a selection of samples from each group) for 60 minutes, bound antibody was detected according to a three step immunoperoxidase method.36,37 Sections were incubated with horseradish peroxidase (HRP) conjugated goat antimouse antibody, followed by incubation with HRP conjugated swine antigoat antibody. HRP activity was detected using hydrogen peroxide as the substrate and 3-amino-9-ethylcarbazole (AEC) as the dye. Slides were counterstained briefly with haematoxylin solution and mounted in Gurr Aquamount (BDH, Poole, UK). Affinity purified, HRP conjugated goat antimouse antibody was obtained from DAKO; affinity purified HRP, conjugated swine antigoat immunoglobulin from Tago (Burlingame, CA, USA); and AEC from Sigma (St Louis, MO, USA).
Dual immunohistochemistry
Dual immunohistochemical labelling was performed as previously described.38,39 In brief, the synovial tissue was incubated with the first primary antibody (anti-RANKL) and subsequent steps, in a standard three step immunoperoxidase method, were performed, developing the final colour product using AEC. Between the first and second immunohistochemical reactions the tissue was washed and blocked with Tris-glycine to prevent cross reaction between the first primary and the second linking antibody. The second primary antibody (anti-CD68, anti-CD55, anti-CD3, or anti-CD22) was placed on the sections overnight at 4°C, followed by a standard immunohistochemical alkaline phosphatase method,37,38 developing the colour reaction with fast blue. No counterstain was used and the sections were mounted in an aqueous mounting medium.
Microscopic analysis
After immunohistochemical staining, sections stained with anti-RANKL were analysed in a random order by computer assisted image analysis, with six high power fields for each section analysed as previously published.36,37,39–41 Two variables were measured by digital image analysis (DIA): (a) integrated optical density (IOD) measured in pixel units, which is a measure of the total amount of staining; (b) mean optical density (MOD), which is a measure of the average density of staining, equivalent to the concentration of protein per cell. In addition, these sections were also scored by a semiquantitative assessment (SQA) method on a five point scale (grades 0–4) by two independent observers in a random order, as described previously.36,37
Statistical analysis
Non-parametric statistics were used to analyse the mean ranks of the SQA scores for the five groups of patients, using a Kruskal-Wallis one way analysis of variance. As the data for area, MOD, and IOD, measured by digital image analysis, were not normally distributed, the data were log transformed and analysed using a one way analysis of variance. Post hoc differences between groups were analysed using Tukey HSD and Bonferroni tests. A value of p<0.05 was considered significant.
RESULTS
Clinical and demographic features
Table 1 presents the clinical and demographic data of the patients with RA and SpA included in the study. The seven patients with OA included five men and two women, with a mean age of 67.4 years (range 56–74), four of whom were taking non-steroidal anti-inflammatory drugs at the time of synovial tissue removal at knee replacement surgery. The 18 normal subjects included 11 men and seven women, with a mean age of 33.3 years (range 18–54).
Immunohistochemistry
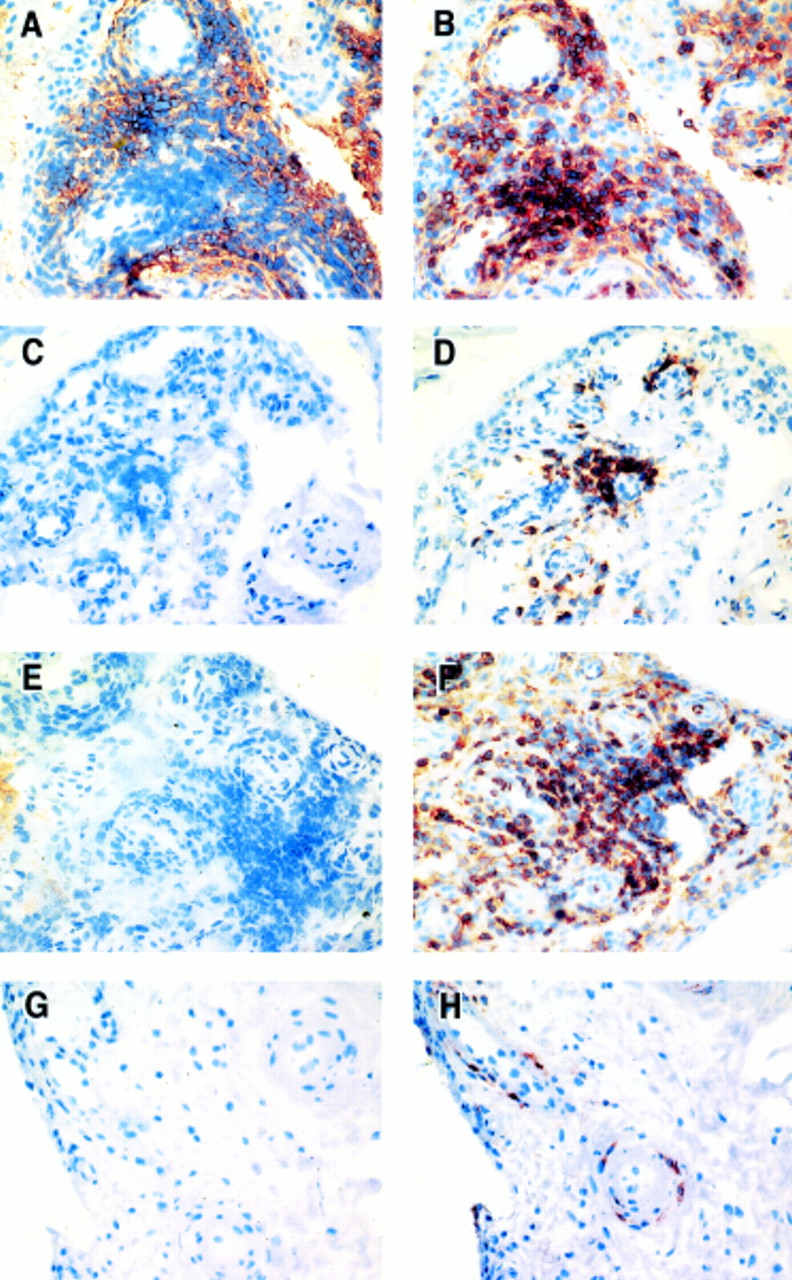
Figures 1A to D shows that the RANKL expression was predominantly seen in areas of mononuclear cell aggregates in the synovial membranes from patients with active RA and SpA, which are absent in patients with inactive RA, OA, and in normal subjects. However, although all samples from the patients with SpA and active RA had active synovitis with lymphoid infiltrates, staining was variable and many sections were negative for RANKL expression. RANKL expression was absent in the RA synovial lining and endothelial cells of the synovial blood vessels in all groups.

RANKL detected with mAb 626/immunoperoxidase and AEC (red), in synovial tissue from a patient with RA with (A) active disease and (B) inactive disease, (C) a patient with SpA, and (D) a patient with OA. (E) to (H) identify cell lineages expressing RANKL (mAb 626/immunoperoxidase (red)) using dual immunohistochemical labelling on serial synovial biopsy sections from a patient with RA with active disease. RANKL expression is identified by mAb 626 using an AEC/immunoperoxidase technique combined with an immunohistochemical alkaline phosphatase technique using fast blue to identify cell surface markers. (E) Dual labelling with anti-CD3 (blue) and both (purple), (F) B cell antibody anti-CD22 (blue), (G) monocyte/macrophage lineage anti-CD68 (blue) and both (purple), (H) FLS with anti- CD55/fast blue (blue). All magnifications taken at ×20.
Dual immunohistochemical labelling with RANKL in combination with lineage-specific mAbs for T cells (CD3), B cells (CD22), macrophages (CD68), and FLS (mAb67), clearly showed that mAb RANKL 626 stained a subset of pan-T cells as well as about 40% of macrophages (figs 1E and G). Neither B cells (CD22) (fig 1F), nor the fibroblasts of the synovial lining (CD55 (mAb67) positive) (fig 1H), co-localised with RANKL positive cells. Activated memory T cells (CD45Ro positive) were abundant in the lymphoid aggregates present in patients with RA and SpA, whereas few were present in the control groups. Regions of CD45Ro cells corresponded with cells both positive and negative for RANKL in sequential sections (fig 2). In tissue sections from the patients with active RA up to about 70% of CD45 positive cells corresponded with cells positive for RANKL. In many cases aggregates of CD45Ro positive cells were devoid of RANKL staining in the corresponding areas of sequentially stained sections.

{kind=link}
{kind=link}
Panels (A), (C), (E), (G) demonstrate RANKL expression, detected with mAb 626/ immunoperoxidase and AEC (red), in synovial tissue from a patient with RA with active disease (A), inactive disease (C), SpA (E), and from a normal subject (G). Panels (B), (D), (F), (H) show sequential sections where CD45Ro is detected with immunoperoxidase and AEC (red) in synovial tissue from patients with active RA (B), inactive RA (D), SpA (F), and from a normal subject (H). All magnifications taken at ×20.
Statistical analysis
Table 2 shows the computer assisted image analysis results and SQA scores for RANKL detected by mAb 626. Expression of RANKL as detected by mAb 626 was seen to varying degrees in all groups of patients. Staining was notably more extensive staining in patients with RA and SpA with active synovitis at the time of synovial biopsy (illustrated in fig 1). There was no significant difference in the RANKL protein expression in the synovial membrane between each group as measured by the SQA. However, there was a trend towards increased RANKL in the groups with active RA and SpA, with some samples graded as 3 or 4 using SQA, whereas RANKL in patients with OA and normal subjects was graded as 0 or 1 in all samples. When assessed with digital image analysis, the total amount of staining (IOD) for RANKL in patients with inactive RA, normal subjects, and patients with OA was significantly less than in those with active RA (p<0.005), although density of staining (MOD) was not significantly different.
Digital image analysis results (IOD and MOD) and mean semiquantitative scores for the expression of RANKL using mAb 626 in synovial tissue from patients with RA, OA, and SpA and normal subjects. Data are shown as mean (SD).
DISCUSSION
Until recently, investigations of bone destruction in RA have implicated inflammatory cytokines, such as IL1α and β, IL6, IL11, and TNFα, as the important mediators stimulating bone lysis.9,10,12 However, there is now mounting evidence that RANKL may be the central mediator of osteoclast development in RA and other bone loss pathologies. The focal role of RANKL is further demonstrated by observation that its natural inhibitor, OPG, completely prevents cartilage and bone loss in an arthritic animal model.42 Although it is still likely that inflammatory mediators present in the RA joint, such as IL1β, IL6, IL11, and IL17, play a part in stimulating bone lysis, their major effects may be indirect through stimulation of RANKL production in the joint.8,14,43
RANK, RANKL, and OPG mRNA are expressed in tissue of the RA joint, and the levels of RANKL, RANK, and OPG are believed to determine whether osteoclastogenesis will occur.5,6,8 The ratio of RANKL to OPG may be a key factor in determining the level of osteoclastic bone resorption.8,19,44 In RA, the infiltration of chronic inflammatory cells, which include macrophages, lymphocytes, and plasma cells, is likely to contribute to osteolysis, directly through differentiation of macrophages into osteoclasts and, indirectly, through release of cytokines that promote osteoclastogenesis and recruitment of macrophages to the joint. Cell culture studies have shown that osteoclasts can form from cells with a macrophage phenotype isolated from the synovium of the RA joint,45 with large numbers rapidly forming from cells isolated from the pannus region.8 The differentiation of these cells is RANKL dependent as demonstrated by its dose dependent inhibition by OPG.46 Our recent work found that the release of OPG protein was significantly reduced in synovial biopsy specimens from patients with active RA compared with control groups.29 This is in accordance with the decreased OPG levels seen in RA synovial fluid compared with OA as measured with an enzyme linked immunosorbent assay (ELISA).19
As far as we know, this study is the first to compare RANKL protein in human synovial tissue from patients with active RA with that seen in patients with inactive RA, SpAs, OA, and in normal subjects using SQA and quantitative (DIA) measurement techniques. This study has shown by immunohistochemistry that RANKL protein is absent or in very low levels in the synovial tissue lining from patients with inactive RA, OA, and from normal patients. This is in agreement with the general observations of Kotake et al, who noted that RANKL positive cells were rare even when OA synovial specimens contained inflammatory cells.19 In our study, although levels varied, RANKL was most abundant in the synovial tissue from patients with RA and SpA with active synovitis. Statistical assessment of SQA showed that RANKL was not significantly higher in the RA or SpA groups than in the control groups, whereas IOD values for RANKL in patients with active RA were significantly more than in inactive RA, OA and normal groups. However, SQA grades were designated according to the proportion of cells, and not the absolute amount of RANKL protein. Therefore, it is likely that we are underestimating the amount of RANKL in the patients with active RA using SQA values when compared with the IOD values. This is supported by previous immunostaining analysis studies, in which an IOD measurement by DIA was shown to be more sensitive to change than SQA.36 Although we were unable to show a significant difference between the groups with active RA and SpA using the IOD values, these values were on average markedly lower in the SpA group than in the group with active RA. Overall, our findings support our original hypothesis that RANKL has an important role in stimulating osteoclast formation and activity in RA joints where bone loss occurs.
We detected RANKL protein in mononuclear aggregates and fibroblast-like cells in the subintimal regions of the synovial membrane. Unlike OPG, RANKL was not expressed on endothelial cells or in the synovial lining.29 Previous studies have shown that activated T cells derived from an RA joint express RANKL mRNA,5 and human activated T cells support differentiation of adherent murine spleen cells18 and human monocytes in coculture.19 It is likely that T lymphocytes support osteoclast differentiation from the many infiltrating cells of the monocyte/macrophage lineage that migrate to the inflamed RA joint. Using dual labelling with a CD3 mAb, we verified that a subset of CD3 positive T cells produces RANKL.19
Previous studies have not reported the production of RANKL by activated, memory T cells in human RA. We found that activated, memory T cells (CD45Ro positive cells) were present in all patient groups but more abundant in the lymphoid aggregates of the patients with RA and SpA. This is in accordance with Sakkas et al, who demonstrated CD45Ro positive cells in OA and RA patient groups, with higher numbers in the RA group.47 A more recent study showed that the high number of CD45Ro and CD68 cells in patients with active RA was reduced in patients attaining clinical remission.48 Sequential staining showed that RANKL coincided with some, but not all, CD45Ro positive cells. This suggests that there are two subpopulations of CD45Ro positive cells that can be distinguished from each other based on their ability to produce RANKL.
The role of B cells in the inflammatory process and bone lysis in RA remains unclear. More recently it has been suggested, using an animal model of inflammatory arthritis, that B lymphoid lineage cells may be able to support osteoclastogenesis through production of RANKL.49 However, our results obtained with human synovial tissue do not support a role for B cells in the production of RANKL as we could not show that RANKL protein was associated with CD22 positive cells.
Previous in vitro studies have shown that cultured synovial fibroblasts, extracted from patients with RA, stimulated with 1,25-dihydroxyvitamin D3, can support osteoclast formation through RANKL expression.6 Occasionally, we noted spindle shaped cells expressing RANKL protein, as also seen by Kotake et al.19 However, in our study cells expressing the fibroblastic cell marker, CD55, did not label with the antibody detecting RANKL protein. Although it is possible that CD55 is not expressed on all fibroblastic cells, we believe that our study supports the contention that activated T lymphocytes, not fibroblasts, are the major cell type that supports osteoclast formation by expressing RANKL in the synovial tissue of patients with active RA.
The current consensus is that monocytes and macrophages are not a major source of RANKL. However, we did observe many cells expressing the macrophage marker CD68 that also expressed RANKL. Without in situ hybridisation we could not verify whether these cells were the source of RANKL or merely binding RANKL that was produced by other cells. However, evidence that these cells can produce RANKL was presented in our previous reports that show that human adherent peripheral blood mononuclear cells in cell culture can express RANKL mRNA when stimulated by prosthetic wear debris.44 Horwood et al also noted macrophage-like cells expressing RANKL mRNA in RA tissue.18
We now have a better understanding of the potential processes and cells involved in joint destruction in RA. In our previous work we showed that OPG is present in endothelial and type A synovial lining cells in the synovial membrane of patients with RA.29 In this study we demonstrated that RANKL protein is associated with macrophages and a subset of CD3 and CD45Ro positive T cells but not B cells or endothelial cells in the RA synovial membrane. The absence of OPG in active RA synovial tissue reported in our previous study, and the significantly higher levels of RANKL in the same tissue demonstrated in this study, show that these molecules are likely to be key regulators of bone loss in active RA. The relative levels of both RANKL and OPG are likely to be important in determining the levels of bone loss in health and disease. OPG is not present in patients with active disease, suggesting that OPG expression may regulate bone loss in RA. This study showed that the highest levels of RANKL protein expression are seen during active disease, further supporting the hypothesis that the extent of bone resorption is largely determined by the relative amounts of RANKL compared with OPG in RA. This identifies OPG/RANKL/RANK pathways as important future therapeutic targets to treat joint destruction in RA.
Acknowledgments
Digital images were prepared with the assistance of Dale Caville from the Department of Pathology, University of Adelaide. Statistical advice was supplied by Flinders University, South Australia.
This study was supported by grants from the National Health and Medical Research Council, Department of Veteran Affairs, Clive and Vera Ramaciotti Foundation, JH and JD Gunn Foundation, and the Rebecca L Cooper Medical Research Foundation.