Article Text

Abstract
Premature death has been long recognised as a manifestation of rheumatoid arthritis (RA). Three lines of evidence can explain why patients with RA die prematurely and why the mortality gap between patients with RA and the general population appears to widening. First, patients with RA have a higher risk of several serious comorbid conditions and they tend to experience worse outcomes after the occurrence of these illnesses. Second, patients with RA do not appear to receive optimal primary or secondary preventive care. And third, the systemic inflammation and immune dysfunction associated with RA appears to promote and accelerate comorbidity and mortality. This paper provides a brief summary and interpretation of the data underlying these findings. Together, these results provide a compelling argument in favour of a focused research programme aimed specifically at eliminating premature death in patients with RA.
Statistics from Altmetric.com
It has been recognised for decades that survival among people with rheumatoid arthritis (RA) is significantly worse than survival in the general population.1–5 Figure 1 shows significantly reduced survival among residents of Rochester, Minnesota, with a first diagnosis of RA between 1955 and 1995 with follow-up to the present, compared with expected survival.

Trends in RA survival over time have also been examined.6 These data disappointingly demonstrate that RA mortality does not appear to have improved over the past three to four decades. When trends in RA mortality are compared with trends in expected mortality in the same population over a long period of time, it is clear that there is a widening mortality gap between patients with RA and the general population. This is because mortality in patients with RA has remained unchanged while mortality in the general population has improved over the past several decades. Thus, overall survival in patients with RA is significantly reduced compared with that in the general population and the mortality gap between RA and the general population appears to be widening over time.
ISCHAEMIC HEART DISEASE
Many recent publications have demonstrated that the excess mortality in patients with RA is largely attributable to cardiovascular disease.7 The most common of these is ischaemic heart disease. In our own studies, ischaemic heart disease has been described according to five distinct constructs: hospitalised myocardial infarction (MI) (defined according to standard epidemiological criteria as definite, probable, suspect or no MI based on the presence of cardiac pain, biomarker values and the Minnesota coding of the electrocardiogram), silent MI (defined by a characteristic electrocardiogram in a non-acute setting), coronary revascularisation procedures (including percutaneous transluminal angioplasty and coronary artery bypass graft), angina pectoris (doctor-defined recognition of cardiac pain in the absence of other causes) and sudden cardiac death (defined as out-of-hospital death occurring in emergency departments, private homes, public places, nursing homes and containing ICD-9 CM codes for 410–414 as the underlying cause of death on death certificates).
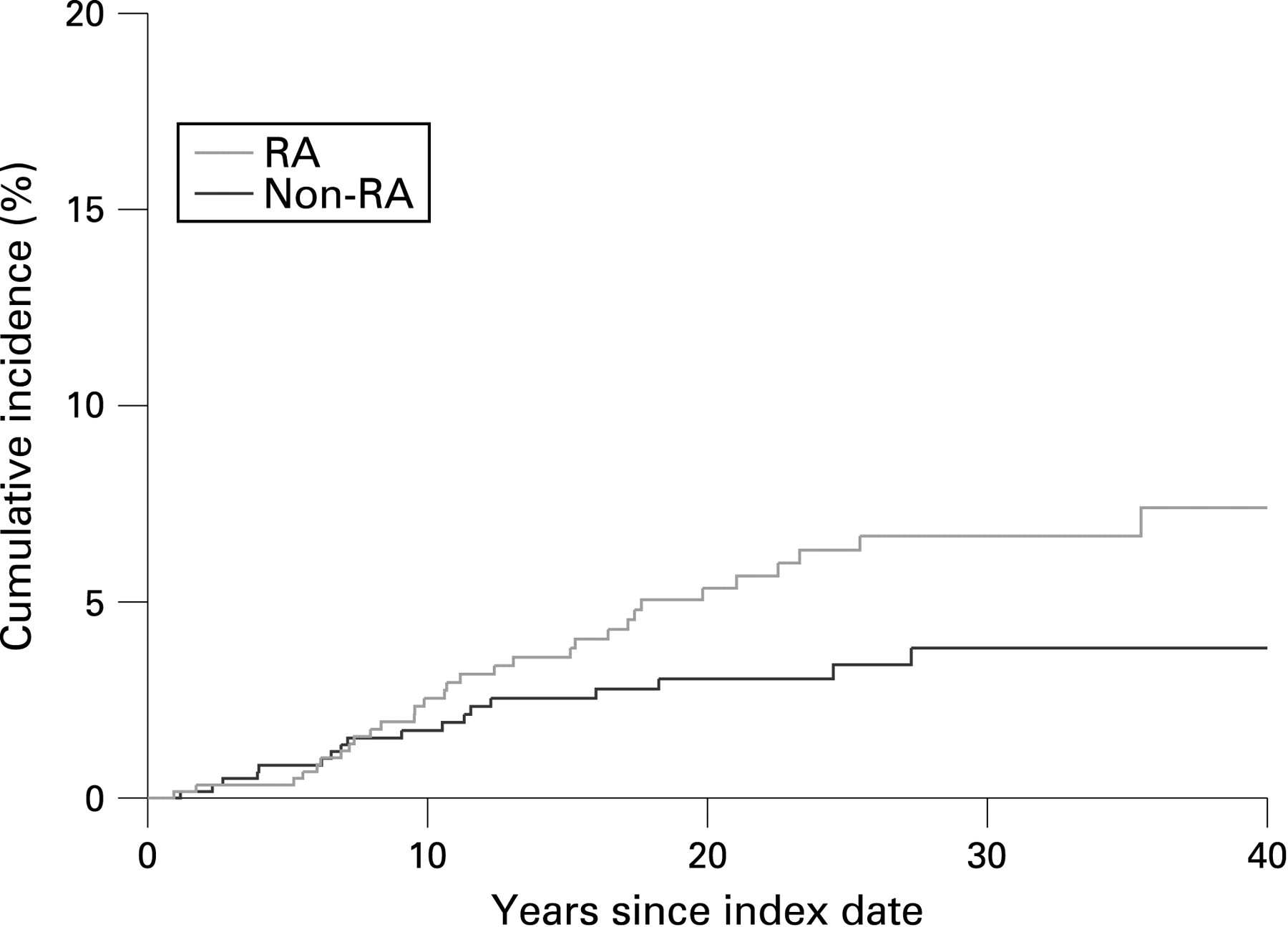
Research from our group and others has repeatedly demonstrated that the risk of ischaemic heart disease is significantly higher among patients with RA than among controls.8–16 We have recently compared the prevalence of ischaemic heart disease in a population-based incidence cohort of 603 patients with RA and a matched non-RA comparison group from the same underlying population. These comparisons demonstrate that at the index date (ie, the date of first fulfilment of the American College of Rheumatology (ACR) RA criteria for patients with RA and a comparable date for non-RA subjects), those with RA are at a more than 3.17-fold higher risk of having had a hospital MI (multivariable odds ratio = 3.17, 95% CI 1.16 to 8.68) and a nearly sixfold increased risk of having had a silent MI (multivariable odds ratio = 5.86, 95% CI 1.29 to 26.64) than those without RA. Our data also demonstrated that the cumulative incidence of silent MI after the incidence/index date continues to rise over time (fig 2). The cumulative incidence of silent MI after 30 years of follow-up, adjusted for competing risks of death, is about 6.0% in the RA and 3.7% in the non-RA cohorts (p = 0.050).

Likewise, the cumulative incidence of sudden death after 30 years of follow-up adjusted again for the competing risk of death by other causes, was 6.7% in the RA and 3.8% in the non-RA cohorts (p = 0.052) (fig 3).

In contradistinction, both the prevalence of angina pectoris at incidence/index date as well as the cumulative risk of angina pectoris after 30 years of follow-up are significantly lower in patients with RA than in the general population.8 Indeed, after 30 years of follow-up, incident angina was identified in only 9.5% of the RA cohort compared with 14% of the non-RA cohort.
In summary, patients with RA are at increased risk of ischaemic heart disease. The increased risk appears to precede the ACR criteria-based diagnosis of RA. The increased risk of ischaemic heart disease may remain silent and may first manifest as sudden cardiac death in patients with RA.
HEART FAILURE
An emerging body of reports now indicate that patients with RA are also at increased risk for heart failure. These studies typically classify heart failure according to the traditional Framingham Heart Study criteria.17 We have previously demonstrated that the cumulative incidence of heart failure after incident RA is statistically significantly higher in patients with RA than in those without the disease in a population-based setting.18
Even after adjusting for competing risks of death, the cumulative risk of heart failure in the RA cohort was significantly higher than in the non-RA cohort throughout follow-up. Indeed, patients with RA reached the same cumulative incidence of heart failure as subjects without RA in about half the time. For example, after 10 years of follow-up, a patient with RA had the same probability of developing heart failure as an age- and-sex matched person without RA after 20 years of follow-up. This effect was constant across all ages. At any particular age, the incidence of heart failure in patients with RA was about twice the incidence in non-RA subjects. Data from multivariable Cox models from our group showed that patients with RA had about twice the risk of developing heart failure and that this risk changed little after accounting for the presence of ischaemic heart disease, other risk factors and the combination of the above (table 1).
In subset analyses, this risk appeared to be largely confined to rheumatoid factor positive RA cases. Indeed, rheumatoid factor positive patients with RA had a risk of developing heart failure that was 2.5 times higher than that of non-RA subjects. Notably, this excess risk of heart failure is similar to that of patients with diabetes mellitus.
Davis and colleagues compared the presentation of heart failure in patients with RA with that in the general population.19 He reported that patients with RA and heart failure presented with a different constellation of signs and symptoms than non-RA subjects with heart failure. In particular, patients with RA and heart failure were less likely to be obese, hypertensive or to have had a history of ischaemic heart disease. Patients with RA and heart failure were also less likely to present with the more typical signs and symptoms of heart failure—that is, they were less likely to be obese, hypertensive or to have a history of ischaemic heart disease. Davis went on to describe echocardiographic features in patients with RA and heart failure compared with non-RA subjects with heart failure. He demonstrated that the proportion of patients with RA and a preserved ejection fraction (⩾50%) was significantly higher for RA than for non-RA subjects with heart failure (58.3% vs 41.4%, p = 0.02). The mean ejection fraction was also shown to be higher among patients with RA than among non-RA subjects (50% vs 43%, p = 0.007; fig 4).

Indeed the likelihood of preserved ejection fraction at the onset of heart failure was 2.57 times more likely in patients with heart failure and with RA than in those without RA (odds ratio = 2.57, 95% CI 1.20 to 5.49). Other investigators also reported that heart failure is more common in patients with RA,20 and a number of echocardiographic series have reported preserved ejection fraction or diastolic functional impairment, or both, in patients with RA.21–23
In summary, patients with RA appear to have an increased risk of heart failure. Heart failure in patients with RA can present in an atypical manner with fewer typical signs and symptoms. People with RA are more likely to have heart failure with preserved ejection fraction.
OTHER COMORBIDITIES
Patients with RA have also been shown to be at increased risk of other important comorbidities. These include infection24 25 and hypertension,26 as well as other conditions.27 There is no evidence that trends in comorbidity among patients with RA, in comparison with subjects without RA, have changed significantly over time (fig 5).

Not only do patients with RA appear to be at increased risk for a number of important comorbidities, but outcome after comborbidities has also been shown to be poorer in patients with RA than in the general population. In our own studies, mortality after MI was significantly higher in subjects with MI and RA than in those with MI who did not have RA (hazard rate for mortality in RA vs non-RA = 1.46, 95% CI 1.01 to 2.10, adjusted for age, sex and calendar year). Likewise, 6-month mortality after heart failure is significantly worse in patients with RA than in non-RA subjects (fig 6). The risk of mortality at 30 days after heart failure was 2.57-fold higher for patients with RA than for non-RA subjects after adjusting for age, sex and calendar year, while the risk of mortality at 6 months after heart failure was 1.94-fold higher for patients with RA than for non-RA subjects after similar adjustment. These comparisons were both highly statistically significant.28

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In summary, there is strong evidence that patients with RA are at high risk for developing several comorbid disorders. Comorbid conditions in patients with RA may have atypical features and thus may be difficult to diagnose. There is no evidence that the excess risks of these comborbidities have declined. Emerging evidence points to poorer outcomes after comorbidity, in patients with RA than in the general population.
PREVENTIVE CARE
Another possible reason why patients with RA continue to die prematurely relates to the use or implementation of preventive care for these patients. Our group reported in 2003 that patients with RA do not receive optimal health maintenance and preventive care services in comparison with their peers in the general population.29 Some years ago our group examined the degree to which patients with RA receive health maintenance and preventive care procedures as recommended by the United States Preventive Services Task Force, a government-appointed independent expert panel whose recommendations are based on systematic review of the evidence of effectiveness of clinical preventive services. Such services include blood pressure testing, lipids profile testing, flu vaccination, pneumococcal vaccination, mammograms and cervical cancer screening. We showed that patients with RA do not receive optimal health maintenance and preventive care services. Davis and colleagues also showed that patients with RA with a clinical diagnosis of heart failure were less likely to undergo echocardiography and less likely to be prescribed cardiovascular drugs—for example, ACE inhibitors, β blockers and diuretics.19 Thus, although only a few studies have examined preventive care in RA, the results do suggest that patients with RA may not receive optimal primary and/or secondary preventive care.
CARDIOVASCULAR RISK FACTORS
A number of investigators have examined the contribution of traditional cardiovascular risk factors and markers of inflammation towards the excess cardiovascular and overall morbidity and mortality in patients with RA.7 30–33 Together these results indicate that while traditional cardiovascular factors are important in patients with RA, they alone do not explain the excess cardiovascular risk in this population. Indeed, some evidence suggests that some risk factors may act differently in patients with RA than in the general population. For example, the balance of cardiovascular risks and potential cardiovascular benefits associated with corticosteroid use may be different in patients with RA than in the general population.34 Also, the benefit of low body mass index (BMI) in cardiovascular protection may be different in patients with RA than in those in the general population because in RA low BMI often reflects disease activity. In addition, inflammatory markers such as erythrocyte sedimentation rate, cyclic citrullinated peptides, rheumatoid factor, large joint swelling, the presence of vasculitis and lung disease are highly significant predictors of cardiovascular outcome and mortality even after adjustment for other confounders.
CONCLUSION
In conclusion, three lines of evidence can explain why patients with RA die prematurely and why the mortality gap between RA and the general population appears to be widening. First, not only do patients with RA have a higher risk of multiple comorbid conditions but also they tend to experience worse outcomes after the occurrence of these comorbid illnesses. Second, patients with RA may not receive optimal primary or secondary preventive care. And third, the systemic inflammation and immune dysfunction associated with RA appears to promote and accelerate comorbidity and mortality. These findings indicate that effective, even optimal control of traditional risk factors alone, while important, will be insufficient to reduce the excess mortality in RA.
To eliminate premature death in patients with RA, a new research strategy is needed that specifically focuses on this goal. Such studies should investigate the role of tight control of inflammation as an intervention and the impact of comorbidity on outcome; and should include large, simple, randomised control trials complemented by well-designed observational studies.
REFERENCES
Footnotes
-
Funding: This work was supported by grants from the National Institutes of Health: R01 AR46849 and AR-30582.
-
Competing interests: None.