Article Text

Abstract
OBJECTIVE To test the efficacy of infliximab in the treatment of patients with severe and active adult onset Still's syndrome (AOSD) despite conventional immunosuppressive therapy.
PATIENTS AND METHODS Six patients with the diagnosis of AOSD according to the Yamagushi criteria of 1992 were treated with infliximab. All patients had severe disease with high clinical and serological activity. Patients were treated initially with high dose steroids or more intensive immunosuppressive therapy. Two patients had a history of multiple disease modifying antirheumatic drug (DMARD) treatments. One patient had a history of three years of AOSD with fever, chills, pleural and pericardial effusions, and hepatosplenomegaly. Despite these treatments, he developed increasing serological signs of inflammation and arthritis of both hips and peripheral joints. Another patient had a history of five years of AOSD with oligoarthritis, myalgias, and recurrent fever despite multiple DMARD treatment, including cyclophosphamide pulse therapy. Our patients with AOSD presented with massive polyarthralgias, polyarthritis, splenomegaly or hepatomegaly, the typical rash, sore throat, weight loss, serositis, continuing fever, leucocytosis, and raised C reactive protein (CRP), erythrocyte sedimentation rate (ESR), and ferritin levels. Four patients with early onset of the disease, fulfilling the diagnostic criteria for AOSD and a clinical and serological high disease activity, were included in our pilot study without any further DMARD treatment apart from the initial steroid treatment. Reduction of established treatment, mainly with steroids, caused a relapse of the disease in all our patients. Patients then received 3–5 mg/kg infliximab on weeks 0, 2, and 6, continuing with intervals of 6–8 weeks depending on the patient's individual disease activity.
RESULTS In all patients, fever, arthralgias, myalgias, hepatosplenomegaly, and the rash resolved after the first courses of treatment with infliximab. All serological variables (CRP, ESR, hyperferritinaemia) returned to normal. After three courses of infliximab infusions, splenomegaly could not be detected in any of our patients. One patient still had severe pain in the left hip caused by hip postarthritic osteoarthrosis, requiring hip replacement. After three courses of treatment with infliximab, splenomegaly could not be detected in any of our patients. Up to now, our patients have received infliximab infusion treatment for between five and 28 months. Throughout this period all patients have continued to benefit from this treatment, with improvement in their clinical symptoms, joint counts, and serological disease activity. One of our patients had a moderate infusion reaction during the second treatment. The infusion was discontinued for one hour and then was resumed with no further problems.
CONCLUSION The disease improved remarkably in all six patients with AOSD after treatment with infliximab, also in the early stage of AOSD. These preliminary data suggest the potential therapeutic benefit of anti-tumour necrosis factor α treatment in AOSD.
- adult onset Still's disease
- tumour necrosis factor α
- infliximab
Statistics from Altmetric.com
Adult onset of Still's disease (AOSD) was first described in 1971 by Bywaters,1 who presented 14 adult patients with features similar to the systemic form of juvenile Still's disease. It is a rare inflammatory rheumatic disease in which the main symptoms are polyarthritis, fever, rash, sore throat, splenomegaly, hepatomegaly, lymphadenopathy, pleuritis, pericarditis, pneumonitis, loss of weight, myalgias,2 ,3 and increased serological signs of inflammation—for example, a raised erythrocyte sedimentation rate (ESR) and C reactive protein (CRP), hyperferritinaemia, and leucocytosis3 ,4; antinuclear antibodies and rheumatoid factors are commonly negative.
About 50% of the patients have a chronic course of the disease, with arthritis being the major cause of chronicity. Although overall prognosis is good, premature death can be caused by complications such as hepatic failure, haemophagocytic syndrome, disseminated intravascular coagulation, amyloidosis, and sepsis. The acute disease is treated with non-steroidal anti-inflammatory drugs and systemic corticosteroids, but when the disease is chronic disease modifying antirheumatic drugs (DMARDs) like methotrexate (MTX), azathioprine (AZA), and cyclophosphamide (CYC) are used. Despite treatment with DMARDs some patients have continuing high disease activity.
In the treatment of rheumatoid arthritis, tumour necrosis factor (TNF) blocking agents, like the chimeric monoclonal antibody cA2, infliximab, have been shown to be effective in patients where DMARDs have failed.5 ,6 Therefore, we investigated the efficacy of infliximab in the treatment of patients with active AOSD.
Methods
Six patients (four female, two male), with a mean age of 42.8 (range 28–60) years and a diagnosis of AOSD according to the Yamagushi criteria of 1992,4 were treated with infliximab in our pilot study. All infectious diseases and other inflammatory rheumatic diseases had been excluded. In addition to the basic patients' data such as age and sex, variables representing the course of disease activity were recorded at each visit: 28 joint score for swollen and tender joints, ESR, CRP, leucocyte counts, ferritin, and body temperature. Clinical symptoms such as rash, splenomegaly, and hepatomegaly, as well as the presence of sore throat, weight loss, and serositis, were also recorded. Two patients underwent further diagnostic examination of inflamed joints by dynamic magnetic resonance imaging (MRI).
Patients were included in our pilot study when they had active disease (see tables 1 and 2) and had previously been treated with high dose corticosteroids or more intensive immunosuppressive therapy. All our six patients had massive polyarthralgias, five had a polyarthritic course of the disease, five continuing fever, five leucocytosis, and five patients showed the typical rash. Splenomegaly was seen in four patients and hepatomegaly in three. Three patients had a sore throat in the initial phase of the disease, three had weight loss, and one patient had a polyserositis. Raised CRP, ESR levels were found in all six patients and hyperferritinaemia in three.
Clinical symptoms of the six patients with adult onset Still's disease. Number of patients is shown
Disease activity variables during infliximab treatment. Results are shown as mean (range)
Two patients had a long course of the disease and had received different DMARD treatments, including MTX, AZA, and CYC pulse therapy, without success. One patient had a history of three years of AOSD with fever, chills, pleural and pericardial effusions, and hepatosplenomegaly. Despite treatment with high dose MTX and corticosteroids, he developed increasing serological signs of inflammation, inflammation of both hips, and peripheral arthritis. A change to AZA 150 mg and pulse corticosteroids did not improve the condition. Another patient had a history of five years of AOSD with oligoarthritis, myalgias, and recurrent fever despite treatment with high dose MTX (up to 40 mg/week), combination treatment with MTX and cyclosporin A (maximal dose 300 mg), CYC pulse therapy, and AZA. Before the start of the infliximab treatment the patient was receiving AZA 200 mg and prednisolone 10 mg. Four further patients with severe AOSD were treated with infliximab after the reduction of corticosteroid treatment caused a relapse of the disease; no further DMARD treatment was given. Patients received 3–5 mg/kg infliximab on weeks 0, 2, and 6, continuing with intervals of 6–8 weeks depending on the patient's individual disease activity. Up to the present, the patients have followed this treatment regimen for between five and 28 months. One patient moved during the observation phase and was lost to follow up. His disease course is reported up to the latest visit to our clinic, which was after five infusions of infliximab.
Results
All our patients benefited from treatment with infliximab. As shown in table 1, fever, myalgias, hepatosplenomegaly, and the rash resolved completely in all patients, and arthritis or arthralgias in five of six. This amelioration of the disease could already be seen after the first courses of treatment with infliximab. All serological variables (CRP, ESR, ferritin values) returned to normal. Also, splenomegaly could not be detected in any of our patients after three courses of infliximab infusions.
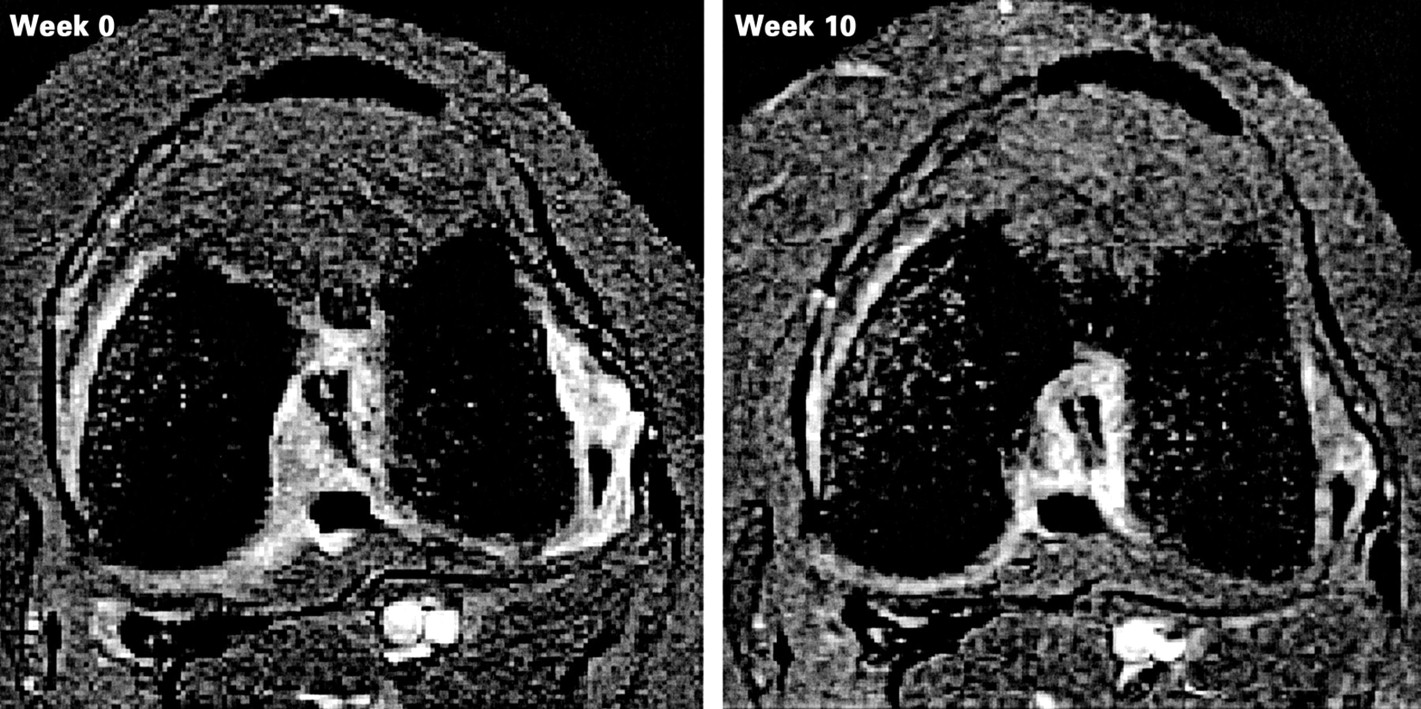
In one of the two patients with a long disease course the swollen joint count was reduced from 30 to 3 and the tender joint count from 33 to 3 one week after the first infliximab infusion. This patient had normal CRP and ESR, no fever, but still had severe pain in the left hip. The reduction in the joint assessment scores was maintained, ESR and CRP returned to baseline levels. MRI of the hips showed decreased gadolinium uptake but marked destruction (fig 1). After changing the DMARD to MTX 25 mg and replacement of both hips, and with continuing infliximab infusions every 6–8 weeks, the ESR and CRP decreased further, and it was possible to reduce the systemic corticosteroid dose to 10–12.5 mg prednisolone.

Magnetic resonance imaging of a patient with both hips inflamed. Improvement in the synovitis is shown by reduction of the gadolinium uptake from week 0 to week 10 after treatment with 5 mg/kg infliximab.
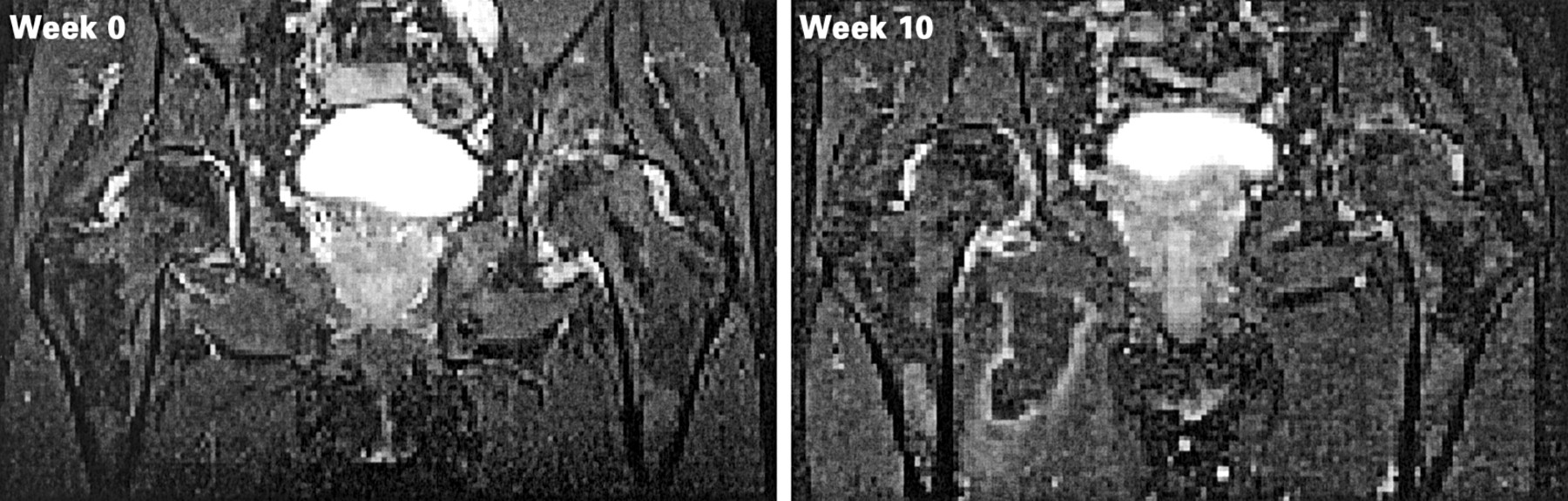
In the patient with a five year history of disease the swollen joint count decreased from 3 to 0, the tender joint count from 7 to 2 after the first infliximab infusion, and the CRP and ESR normalised. Moreover, fever is still absent. An MRI scan of the left knee showed reduced gadolinium uptake after 10 weeks (fig 2). With infliximab infusion intervals of eight weeks, the arthritis has remained in remission.
{kind=link}
{kind=link}
Magnetic resonance imaging of a patient's left inflamed knee joint. The change in gadolinium uptake from week 0 to week 10 after treatment with 5 mg/kg infliximab is shown. The complete reduction of gadolinium uptake indicates a marked improvement of the synovitis.
Up to the present, our patients have received infliximab infusion treatment for between five and 28 months. Throughout this period their clinical symptoms, joint counts, and serological disease activity have improved (tables 1 and 2).
One patient had a moderate infusion reaction during the second treatment. The infusion was discontinued for one hour and then resumed with no further problems.
Two patients are receiving concomitant treatment with MTX (10–15 mg/week), one patient with AZA 100 mg/day, and two patients receive low dose corticosteroids (<10 mg/day).
Discussion
As in other chronic inflammatory rheumatic diseases like rheumatoid arthritis or, as recently reported, in ankylosing spondylitis,7 treatment with antagonists against TNFα like the monoclonal chimeric antibody, infliximab, seems to be a very effective alternative for the treatment of the rare disease, AOSD. Our experience with this treatment in this small cohort of patients shows, besides the striking potency of this new drug, good tolerability. None of our patients had to stop treatment. This is of particular interest as severe disease and even death can occur.8 ,9 Prognostic markers have not been identified so far.9 Thus this regimen may be an alternative to conventional treatment for patients with severe and highly active AOSD who relapse after an initial treatment with high dose corticosteroids or in whom DMARDs are either ineffective or produce side effects, in the initial course of the disease. Of course, these preliminary data require confirmation in larger studies.