Article Text

Abstract
Objectives Biological disease-modifying antirheumatic drugs (bDMARDs) have shown diminished clinical response following an inadequate response (IR) to ≥1 previous bDMARD. Here, tofacitinib was compared with placebo in patients with an IR to conventional synthetic DMARDs (csDMARDs; bDMARD-naive) and in patients with an IR to bDMARDs (bDMARD-IR).
Methods Data were taken from phase II and phase III studies of tofacitinib in patients with rheumatoid arthritis (RA). Patients received tofacitinib 5 or 10 mg twice daily, or placebo, as monotherapy or with background methotrexate or other csDMARDs. Efficacy endpoints and incidence rates of adverse events (AEs) of special interest were assessed.
Results 2812 bDMARD-naive and 705 bDMARD-IR patients were analysed. Baseline demographics and disease characteristics were generally similar between treatment groups within subpopulations. Across subpopulations, improvements in efficacy parameters at month 3 were generally significantly greater for both tofacitinib doses versus placebo. Clinical response was numerically greater with bDMARD-naive versus bDMARD-IR patients (overlapping 95% CIs). Rates of safety events of special interest were generally similar between tofacitinib doses and subpopulations; however, patients receiving glucocorticoids had more serious AEs, discontinuations due to AEs, serious infection events and herpes zoster. Numerically greater clinical responses and incidence rates of AEs of special interest were generally reported for tofacitinib 10 mg twice daily versus tofacitinib 5 mg twice daily (overlapping 95% CIs).
Conclusions Tofacitinib demonstrated efficacy in both bDMARD-naive and bDMARD-IR patients with RA. Clinical response to tofacitinib was generally numerically greater in bDMARD-naive than bDMARD-IR patients. The safety profile appeared similar between subpopulations.
Trial registration numbers (NCT00413660, NCT0050446, NCT00603512, NCT00687193, NCT00960440, NCT00847613, NCT00814307, NCT00856544, NCT00853385).
- DMARDs (biologic)
- DMARDs (synthetic)
- Rheumatoid Arthritis
- Anti-TNF
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Video abstract
Introduction
Increasing evidence suggests that early, aggressive intervention has a beneficial impact on the clinical response to therapy in patients with rheumatoid arthritis (RA), and delay in initiation of treatment and prior disease-modifying antirheumatic drug (DMARD) exposure has been associated with decreased response.1–9 Although there are limited data in randomised controlled trials on the efficacy treatment in biological DMARD (bDMARD)-naive patients versus patients with an inadequate response (IR) to bDMARDs (bDMARD-IR), published reports of bDMARDs have generally shown less clinical response when a bDMARD is used after an IR to at least one previous bDMARD.10–21 It is important that new RA therapies demonstrate efficacy and tolerability in RA patient populations with varying disease duration and prior treatment exposure to reflect the variability seen in clinical practice.
Tofacitinib is an oral Janus kinase inhibitor for the treatment of RA. The clinical efficacy and safety of tofacitinib 5 and 10 mg twice daily as monotherapy or in combination with conventional synthetic DMARDs (csDMARDs) for the treatment of RA has been reported previously in phase II,22–26 phase III27–32 and long-term extension (LTE) clinical studies.33
Patients receiving tofacitinib in the RA development programme included those who were naive to or had an IR to bDMARDs. The objectives of these analyses were to compare the efficacy and safety of tofacitinib 5 and 10 mg twice daily versus placebo in patients who had an IR to csDMARDs only (bDMARD-naive), and patients with an IR to previous bDMARDs including tumour necrosis factor inhibitors (TNFi; bDMARD-IR).
Methods
Clinical studies
Phase II studies
The four phase II studies were randomised, double-blind, placebo-controlled studies: A3921025 (NCT00413660), A3921035 (NCT00550446), A3921039 (NCT00603512) and A3921040 (NCT00687193). Patients received tofacitinib 1, 3, 5, 10 or 15 mg twice daily, tofacitinib 20 mg once daily (A3921025) or placebo, as monotherapy (A3921035 and A3921040) or in combination with background methotrexate (A3921025 and A3921039). A3921035 included a monotherapy adalimumab arm. Patients had an IR to a bDMARD or csDMARD (A3921035 and A3921040), or methotrexate (A3921025 and A3921039). Full details have been published previously.22 ,24–26
Phase III studies
The five phase III studies were double-blind, placebo-controlled, global studies: ORAL Step (A3921032; NCT00960440), ORAL Scan (A3921044; NCT00847613), ORAL Solo (A3921045; NCT00814307), ORAL Sync (A3921046; NCT00856544) and ORAL Standard (A3921064; NCT00853385). Patients had an IR to a bDMARD or csDMARD (ORAL Solo and ORAL Sync), methotrexate (ORAL Scan and ORAL Standard) or TNFi (ORAL Step). Patients with RA received tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily or placebo, as monotherapy (ORAL Solo), with background csDMARDs (ORAL Sync) or with background methotrexate (ORAL Standard, ORAL Scan, ORAL Step). ORAL Standard included an adalimumab plus methotrexate arm. In ORAL Sync, ORAL Standard and ORAL Scan, placebo patients who did not achieve ≥20% decrease in tender/swollen joints were treated with tofacitinib at month 3. All remaining placebo patients were treated with tofacitinib at month 6. In ORAL Step and ORAL Solo, all placebo patients were treated with tofacitinib at month 3. Full details have been published previously.27–31 After the publication of ORAL Standard, one of its study sites (nine patients randomised) was found to be non-compliant to study procedures and those patients have been removed from the efficacy analyses presented here.
Patient subpopulations
IR was defined as discontinuation due to lack of efficacy, an adverse event (AE), or both, in all studies except for study A3921039, which did not collect the same detailed information.
Two analysis cohorts were included: pooled phase II and phase III studies (P2/P3) cohort, and the pooled phase III studies (P3) cohort. The P2/P3 cohort included patients from the four phase II and five phase III studies. The P3 cohort included patients from the five phase III studies.
The following patient subpopulations were analysed in both P2/P3 and P3 cohorts according to prior DMARD experience and response to DMARD therapy:
bDMARD-naive: patients who had an IR to csDMARDs only
bDMARD-IR: patients with an IR to previous TNFi or other bDMARDs.
For the P2/P3 cohort, the following patient subpopulations were analysed according to previous TNFi exposure:
bDMARD-naive: patients who had an IR to csDMARDs only
patients who were IR to one previous TNFi
patients who were IR to multiple previous TNFi (≥2 previous TNFi).
Efficacy and safety analyses
The following efficacy parameters were assessed: American College of Rheumatology (ACR) 20/50/70 response rates; disease activity score (DAS)28-4(erythrocyte sedimentation rate) (ESR); Health Assessment Questionnaire-Disability Index (HAQ-DI); Clinical Disease Activity Index (CDAI) and Simplified Disease Activity Index (SDAI). Efficacy comparisons were performed on the P2/P3 cohort at months 3 and 6.
Safety parameters assessed using exposure estimates and incidence rates (patients with event per 100 patient-years of observation) included discontinuations due to AEs; serious AEs (SAEs); all-cause mortality; malignancies (excluding non-melanoma skin cancer (NMSC)); lymphoma/lymphoproliferative disorders; all herpes zoster (HZ; serious and non-serious); serious HZ; serious infection events (SIEs); tuberculosis (TB); opportunistic infections (excluding TB) and major adverse cardiovascular events. Safety was assessed in the P3 cohort during months 0–6 for placebo and months 0–24 for tofacitinib. Patients initially treated with placebo were counted in the placebo group until treatment with tofacitinib. Safety endpoints were analysed in the P3 cohort only and not the P2/P3 cohort due to the phase II studies containing multiple doses and titrations of tofacitinib, thereby making it difficult to assign a safety event to a specific tofacitinib 5 or 10 mg twice daily dose.
Statistical analyses
All efficacy and safety analyses were based on the full analyses set—all patients who were randomised and received ≥1 dose of study treatment (tofacitinib or placebo).
For binary efficacy variables, missing values were computed using non-responder imputation, except for CDAI and SDAI (low-disease activity or remission) where observed case data were used. Testing for treatment differences between tofacitinib and placebo was based on the normal approximation. For continuous variables, missing values were handled by the linear mixed-effect models (used to assess the treatment effects). For the exploratory analysis of tofacitinib versus placebo at month 3, statistical significance was declared at p<0.05, without multiplicity corrections to preserve type I error.
The 95% CIs were presented for the bDMARD-naive and bDMARD-IR subpopulations. For binary efficacy variables, exact binomial intervals were calculated, and for continuous efficacy variables, normal approximation was used.
All safety analyses were based on observed cases. Incidence rates for safety parameters were calculated by exposure and dose. Incidence rates were based on the number of patients with an event and total exposure time censored at time of event, death or withdrawal from the study; 95% CIs for incidence rates were based on maximum likelihood estimation. A subanalysis of incidence rates for safety events of special interest for patients with/without concomitant glucocorticoid treatment was also performed.
Results
Patients
A total of 1071, 1090 and 651 bDMARD-naive patients were randomised to receive tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily and placebo, respectively. In the bDMARD-IR subpopulation, 259, 253 and 193 patients were randomised to receive tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily and placebo, respectively. In the bDMARD-IR group, discontinuations of prior bDMARDs occurred due to lack of efficacy (68.4%), AEs (7.2%) and both lack of efficacy and AEs (24.4%).
Baseline demographics and disease characteristics were generally similar for tofacitinib versus placebo groups (table 1). Compared with bDMARD-naive patients, a higher proportion of bDMARD-IR patients were Caucasian, had a higher mean body mass index, were from the USA, had longer mean disease duration and slightly greater mean disease activity at baseline (table 1). Compared with bDMARD-IR patients, higher proportions of bDMARD-naive patients were from Latin America or rest of world, had previously taken csDMARDs other than methotrexate and were rheumatoid factor positive (table 1).
Patient demographics and baseline disease characteristics in the P2/P3 cohort
Efficacy
Tofacitinib 5 mg twice daily
Tofacitinib 5 mg twice daily versus placebo
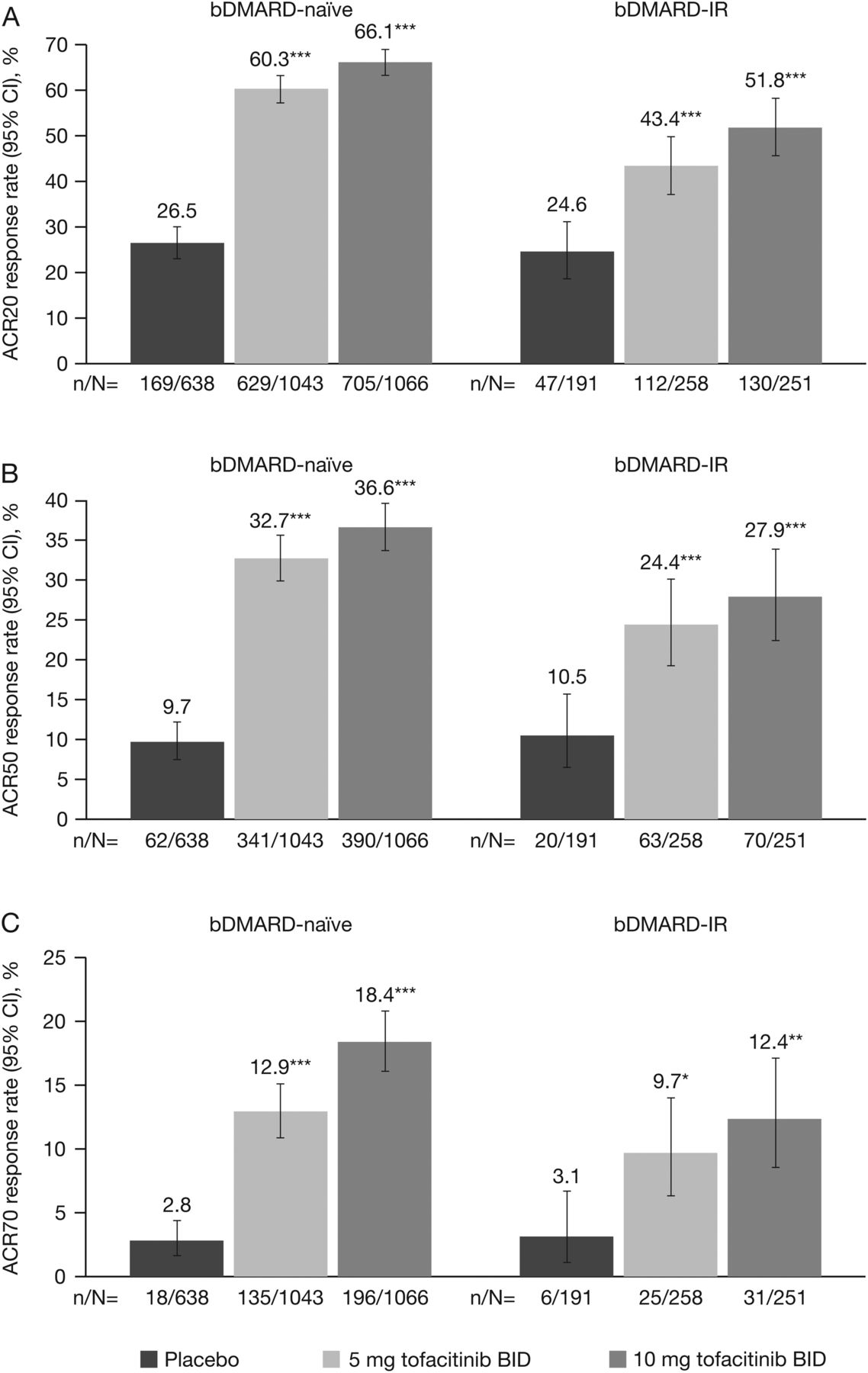
In both bDMARD-naive and bDMARD-IR patients, a significantly (p<0.05) greater proportion of patients in the tofacitinib 5 mg twice daily group versus placebo achieved ACR20/50/70 response rates at month 3 (figure 1). Furthermore, least-squares mean changes from baseline at month 3 in HAQ-DI and DAS28-4(ESR) (figure 2), and improvements in other efficacy parameters, were significantly (p<0.05) higher for tofacitinib 5 mg twice daily versus placebo, except the percentage of patients achieving improvements ≥0.22 in HAQ-DI for bDMARD-IR patients (table 2).
Efficacy responses at month 3 for bDMARD-naive versus bDMARD-IR in the P2/P3 cohort

(A) ACR20, (B) ACR50 and (C) ACR70 response rates (95% CI) at month 3 for bDMARD-naive versus bDMARD-IR populations in phase (P)2/P3 cohort (FAS, NRI). *p<0.05; **p<0.001; ***p<0.0001 vs placebo. No preservation of type I error or multiple-comparisons correction was applied to p values as statistical significance defined as p<0.05 was exploratory in nature; 95% CIs are exact binomial confidence intervals for single proportion. ACR 20/50/70, proportion of patients achieving >20%, >50%, and >70% improvement in American College of Rheumatology criteria; bDMARD, biologic disease-modifying antirheumatic drug; BID, twice daily; CI, confidence interval; FAS, full analysis set; IR, inadequate responders; NRI, non-responder imputation.

{kind=link}
{kind=link}
LS mean change from baseline (95% CI) at month 3 in (A) HAQ-DI and (B) DAS28-4(ESR) for bDMARD-naive versus bDMARD-IR populations in the phase (P)2/P3 cohort (FAS, longitudinal model). ***p<0.0001 vs placebo. No preservation of type I error or multiple-comparisons correction was applied to p values as statistical significance defined as p<0.05 was exploratory in nature; 95% CIs are based on normal approximation. bDMARD, biologic disease-modifying antirheumatic drug; BID, twice daily; CI, confidence interval; DAS, disease activity score; ESR, erythrocyte sedimentation rate; FAS, full analysis set; HAQ-DI, Health Assessment Questionnaire-Disability Index; IR, inadequate responders; LS, least squares.
Tofacitinib 5 mg twice daily versus placebo by prior TNFi exposure
For the bDMARD-naive subpopulation, improvements were significantly (p<0.05) greater for tofacitinib 5 mg twice daily versus placebo across all efficacy endpoints at month 3 (see online supplementary table S1). In the 1 and ≥2 previous TNFi groups, tofacitinib 5 mg twice daily resulted in significant (p<0.05) improvements versus placebo in efficacy endpoints at month 3, except DAS28-4(ESR)≤3.2 and <2.6, and HAQ-DI ≤0.5 for one previous TNFi, and ACR70, CDAI≤10 and ≤2.8, HAQ-DI≤0.5 and SDAI≤11 for ≥2 previous TNFi, although all responses were numerically higher for tofacitinib versus placebo (see online supplementary table S1).
Tofacitinib 5 mg twice daily bDMARD-naive versus bDMARD-IR analyses
At months 3 and 6, improvements in clinical responses were numerically greater for bDMARD-naive versus bDMARD-IR patients, except SDAI≤3.3 at month 3 and DAS28-4(ESR)≤3.2 at month 6; 95% CIs were overlapping for most efficacy parameters, except ACR20 at month 3 (figure 1; tables 2 and 3).
Efficacy responses at month 6 for bDMARD-naive versus bDMARD-IR in the P2/P3 cohort (FAS, NRI)
At month 3, improvements in clinical responses were numerically greater for bDMARD-naive patients versus one previous TNFi patient versus ≥2 previous TNFi patients for tofacitinib 5 mg twice daily, except CDAI and SDAI remission endpoints; 95% CIs were overlapping for most efficacy parameters, except ACR20 (see online supplementary table S1).
Tofacitinib 10 mg twice daily
Tofacitinib 10 mg twice daily versus placebo
In both bDMARD-naive and bDMARD-IR patients, improvements in all efficacy parameters were significantly (p<0.05) greater for tofacitinib 10 mg twice daily versus placebo (figures 1 and 2 and table 2).
Tofacitinib 10 mg twice daily versus placebo by prior TNFi exposure
For the bDMARD-naive, and 1 and ≥2 previous TNFi groups, improvements were significantly (p<0.05) greater for tofacitinib 10 mg twice daily versus placebo across all efficacy endpoints at month 3, except ACR70, CDAI≤10 and ≤2.8, and DAS28–4(ESR)<2.6 for ≥2 previous TNFi, although all responses were numerically higher for tofacitinib versus placebo (see online supplementary table S1).
Tofacitinib 10 mg twice daily bDMARD-naive versus bDMARD-IR analyses
At months 3 and 6, improvements in clinical responses were numerically greater for bDMARD-naive versus bDMARD-IR patients, except DAS28-4(ESR)<2.6 at month 6; 95% CIs were overlapping for most efficacy parameters, except ACR20 at month 3 (figures 1 and 2; tables 2 and 3).
Improvements in clinical responses at month 3 were numerically greater for all efficacy parameters for bDMARD-naive patients versus one previous TNFi patient versus ≥2 previous TNFi patients with the following exceptions: SDAI<11 and LS mean change from baseline in HAQ-DI (in bDMARD-naive and one previous TNFi group); LS mean change from baseline in DAS28-4(ESR) (in bDMARD-naive and ≥2 previous TNFi groups) ACR20 (in one previous TNFi and ≥2 previous TNFi groups); 95% CIs were overlapping for most efficacy parameters, except ACR20 (see online supplementary table S1).
Safety: tofacitinib 5 mg twice daily and tofacitinib 10 mg twice daily
Incidence rates were numerically higher for both tofacitinib doses versus placebo for SIEs, HZ and malignancies (excluding NMSC); bDMARD-IR versus bDMARD-naive subpopulations for discontinuations due to AEs, HZ and malignancies (excluding NMSC) (table 4). Despite the noted numerical differences, 95% CIs were generally overlapping when comparing each tofacitinib dose versus placebo within each subpopulation. The CIs of incidence rates for safety events in the placebo and bDMARD-IR groups were wider versus the bDMARD-naive tofacitinib groups due to the lower total exposure (table 4).
Incidence rates (patients with event per 100 patient-years; 95% CI) for safety events of special interest in bDMARD-naive versus bDMARD-IR subpopulations in the P3 cohort
Patients who received glucocorticoids had a higher incidence rate of SAEs, discontinuation due to AEs, SIEs and HZ versus patients who did not receive glucocorticoids (see online supplementary table S2). No differences in baseline demographics or efficacy were observed between the two subpopulations (data not shown).
Discussion
To the best of our knowledge, this is the first study to analyse the efficacy and safety of an approved RA treatment in bDMARD-naive versus bDMARD-IR populations using pooled data from a large, randomised clinical trial programme.
Tofacitinib was effective in reducing the signs and symptoms of RA when used before or after bDMARDs. In both bDMARD-naive and bDMARD-IR patients in the P2/P3 cohort, improvements in efficacy parameters at month 3 were significantly (p<0.05) greater for both tofacitinib doses versus placebo (except improvements ≥0.22 in HAQ-DI for bDMARD-IR patients who received tofacitinib 5 mg twice daily). In general, improvements in clinical responses at months 3 and 6 were numerically greater for bDMARD-naive versus bDMARD-IR patients, with overlapping 95% CIs. In particular, the proportions of patients achieving ACR20/50/70 responses were higher in the bDMARD-naive versus the bDMARD-IR subpopulation; the differences between the subpopulations for endpoints such as changes in DAS28-4(ESR), CDAI or SDAI, or achieving DA28-4(ESR), CDAI or SDAI remission or low-disease activity were less prominent. Of note, bDMARD-IR patients had longer disease duration and slightly greater disease activity at baseline compared with bDMARD-naive patients, which could have influenced these results. Although no formal comparisons were made, numerically greater clinical responses were generally reported for tofacitinib 10 mg twice daily versus tofacitinib 5 mg twice daily; however, both tofacitinib doses reported significant improvements versus placebo across efficacy endpoints in both subpopulations.
Improvements in efficacy parameters were similar in bDMARD-IR tofacitinib-treated patients compared with TNFi-IR tofacitinib-treated patients from the ORAL Step study; this was expected given that these analyses included ORAL Step tofacitinib-treated patients (n=399).27 In bDMARD-IR subpopulations treated with tofacitinib, ACR and DAS response rates at months 3 and 6 were generally similar to those reported for non-TNFi bDMARDs, including abatacept, rituximab and tocilizumab in TNFi-IR patients, except DAS endpoints for tocilizumab 8 mg/kg.10 ,13 ,14 In bDMARD-naive patients treated with tofacitinib, clinical efficacy endpoints were generally similar to those reported for bDMARDs in patients who were bDMARD-naive or with early RA.9 ,34–41
More patients achieved efficacy endpoints at month 3 when treated with tofacitinib compared with placebo even after patients were stratified by exposure to previous TNFi. While tofacitinib was significantly greater versus placebo in patients exposed to bDMARDs for many endpoints, patients with ≥2 previous TNFi exposure generally had poorer efficacy responses than bDMARD-naive patients and those with one previous TNFi exposure. The number of patients in the multiple TNFi group was less than the other TNFi exposure groups; for several endpoints, responses were numerically higher but not statistically significant for tofacitinib versus placebo in the multiple TNFi group—possibly attributable to the smaller sample sizes for each treatment group, therefore, conclusions must be made with caution. Baseline differences between the groups may impact on the differences in efficacy observed. Nevertheless, data in tofacitinib-treated bDMARD-IR patients were consistent with studies of bDMARDs that have generally shown less clinical response when a bDMARD is used after an IR to at least one previous bDMARD.10–21 Stratification by prior TNFi exposure also showed that ACR response rates in tofacitinib-treated bDMARD-IR patients were generally similar to non-TNFi bDMARDs,10 ,13 ,14 ,19 ,20 but greater than TNFi.11 ,12 ,18–21 The results of these analyses suggest that tofacitinib demonstrates efficacy compared with placebo in patients, irrespective of prior TNFi exposure; results were generally similar to those observed for bDMARDs.
In the P3 cohort, the tofacitinib safety profile appeared similar between treatment groups and between bDMARD-naive and bDMARD-IR subpopulations of patients with RA, with incidence rates that had overlapping 95% CIs. Incidence rates for safety events were generally numerically higher for both tofacitinib doses versus placebo and tofacitinib 10 mg twice daily versus tofacitinib 5 mg twice daily for SIEs, HZ and malignancies (excluding NMSC), and in the bDMARD-IR versus bDMARD-naive subpopulations for discontinuations due to AEs, SAEs, HZ and malignancies (excluding NMSC). Patients that received glucocorticoids had a higher incidence of SAEs, discontinuation due to AEs, SIEs and HZ (all serious HZ occurred in patients receiving glucocorticoids); consistent with reports from RA patient databases of bDMARDs.42 ,43 Opportunistic infections (excluding TB), TB, malignancies, lymphoma/lymphoproliferative disorders and deaths were uncommon in both bDMARD-naive and bDMARD-IR tofacitinib-treated patients in the P3 cohort; higher rates were observed for tofacitinib 10 mg twice daily versus tofacitinib 5 mg twice daily, except deaths (overlapping 95% CIs). There is no apparent or consistent association between tofacitinib dose and risk of malignancy.44 In phase III studies, nearly all TB cases occurred in regions of high TB endemicity.45 Similar to the bDMARD-IR subpopulation, these safety events were also uncommon in the tofacitinib ORAL Step study27 and studies of bDMARDs in TNFi-IR populations.10 ,11 ,13 ,14 Compared with tofacitinib-treated patients in the bDMARD-naive subpopulation, these safety events of special interest were generally similar to those reported for bDMARDs in patients who were bDMARD-naive or with early RA.9 ,34–41 ,46 The safety and efficacy profiles in bDMARD-naive and bDMARD-IR patients in the randomised controlled trials were generally similar to the data from tofacitinib LTE studies to date (data not shown47).
These pooled analyses provide a large data set for tofacitinib treatment groups in bDMARD-naive and bDMARD-IR subpopulations. The limitations of the pooling of data from studies with different designs and methodology may result in a heterogeneous patient population (despite similar inclusion/exclusion criteria), making it difficult to detect changes due to larger variations in the analysed populations. As patients were treated with placebo only for a short term, the placebo group had fewer patients and less exposure than the tofacitinib group in phase III studies, resulting in sample size differences for the comparisons at month 3. The studies included in these analyses were not designed for comparisons between bDMARD-naive and bDMARD-IR patients and patients with/without concomitant glucocorticoids; patients were not randomised according to this stratification, no formal statistical analyses were performed to compare efficacy or safety between these subpopulations, and conclusions were based on descriptive analyses only.
In summary, tofacitinib was effective in reducing the signs and symptoms of RA when used before or after bDMARDs. With a few exceptions, tofacitinib treatment resulted in greater efficacy responses in bDMARD-naive versus bDMARD-IR patients. The tofacitinib safety profile appeared similar between subpopulations. Taken together, these results suggest that tofacitinib provides an effective treatment option for both bDMARD-naive and bDMARD-IR patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Tore K Kvien
Contributors KK, TH and EB were involved in conception and design of the study/analyses. KK performed data and statistical analyses. CC-S, GB, PN, CAFZ, and RF were involved in data acquisition during the phase II, phase III and long-term extension clinical studies. CC-S, GB, PN, CAFZ, KS, KK, TH, EB and RF were involved in data interpretation and manuscript drafting, reviewing and development.
Funding This study was sponsored by Pfizer. Anne Marie Reid, PhD, of Complete Medical Communications provided editorial support under the guidance of the authors and was funded by Pfizer. Lisy Wang, Ryan DeMasi and Andrew Anisfeld, all employees and shareholders of Pfizer, provided intellectual input during the manuscript development.
Competing interests CC-S, PN, CAFZ and RF have received research grants and consultancy fees from Pfizer. GB is a member of the Speaker's Bureau for and has received research grants and consultancy fees from Pfizer. KS, KK, TH and EB are employees and shareholders of Pfizer.
Patient consent Obtained.
Ethics approval All studies were approved by the Institutional Review Boards (IRBs) and/or Independent Ethics Committees of each investigational centre or a central IRB. The studies were conducted in compliance with the Declaration of Helsinki and the International Conference on Harmonisation Good Clinical Practice Guidelines.
Provenance and peer review Not commissioned; externally peer reviewed.