Article Text

Abstract
Objective In the general population, the incidence of stroke is increased following other serious events and hospitalisation. We investigated the impact of serious adverse events on the risk of stroke in patients with rheumatoid arthritis (RA), taking risk factors and treatment into account.
Methods Using data of the German biologics register RABBIT (Rheumatoid Arthritis: Observation of Biologic Therapy) with 12354 patients with RA, incidence rates (IRs) and risk factors for stroke were investigated using multi-state and Cox proportional hazard models. In addition, in a nested case–control study, all patients with stroke were matched 1:2 to patients with identical baseline risk profile and analysed using a shared frailty model.
Results During follow-up, 166 strokes were reported. The overall IR was 3.2/1000 patient-years (PY) (95% CI 2.7 to 3.7). It was higher after a serious adverse event (IR: 9.0 (7.3 to 11.0)), particularly within 30 days after the event (IR: 94.9 (72.6 to 121.9)). The adjusted Cox model showed increased risks of age per 5 years (HR: 1.4 (1.3 to 1.5)), hyperlipoproteinaemia (HR: 1.6 (1.0 to 2.5)) and smoking (HR: 1.9 (1.3 to 2.6)). The risk decreased with better physical function (HR: 0.9 (0.8 to 0.96)). In the case–control study, 163 patients were matched to 326 controls. Major risk factors for stroke were untreated cardiovascular disease (HR: 3.3 (1.5 to 7.2)) and serious infections (HR:4.4 (1.6 to 12.5)) or other serious adverse events (HR: 2.6 (1.4 to 4.8)).
Conclusions Incident adverse events, in particular serious infections, and insufficient treatment of cardiovascular diseases are independent drivers of the risk of stroke. Physicians should be aware that patients who experience a serious event are at increased risk of subsequent stroke.
- rheumatoid arthritis – stroke – cerebrovascular events - serious adverse events – multi state models
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- rheumatoid arthritis – stroke – cerebrovascular events - serious adverse events – multi state models
Introduction
Cerebrovascular diseases are a major health concern worldwide representing the second most common cause of death and the most frequent reason for disability.1 Two main types are distinguished—ischaemic and haemorrhagic strokes—depending on their aetiology. In the general population, risk factors for stroke are divided into non-modifiable such as age, gender, family predisposition or genotype and modifiable such as management of underlying comorbidities (eg, hypertension) or life-style (eg, smoking).2 3 Recently, elevated levels of the cytokines tumour necrosis factor (TNF)-alpha and interleukin 6, as well as of high-sensitivity C reactive protein (CRP) were discussed additionally as ischaemic stroke promoters.3
Compared with the general population, the risk of stroke is higher in patients with rheumatoid arthritis (RA). A recently published meta-analysis states significantly higher risks for ischaemic (OR: 1.64) and haemorrhagic (OR: 1.68) strokes in patients with RA.4 Nonetheless, investigations of risk factors for stroke in RA are scarce. In a matched case–control study, ischaemic stroke was predicted by RA severity and prevalent comorbidities.5 Other authors identified elevated erythrocyte sedimentation rate (ESR)6 7 and CRP values7 as risk factors for ischaemic stroke.
Novel approaches in the general population have taken precedent adverse events (AEs) into account and showed significant associations of incident stroke with infections,8 9 hospitalisation10 and cancer.11 The authors hypothesised pathogenic mechanisms of serious infections, dehydration during hospitalisation and pathophysiological complications of cancer as triggering events for stroke.
These findings suggest that prior AEs should also be considered in RA as possible triggers for stroke in addition to known risk factors. Calabrese et al 12 found a time-dependent risk for stroke after herpes zoster, being highest within the first 90 days after diagnosis. So far, it is unclear whether similar mechanisms or pathways also apply to other AEs in patients with RA.
The aim of our study was to investigate risk factors for non-haemorrhagic stroke in patients with RA using data of a large observational cohort study. We were interested in the impact of RA-specific disease characteristics such as inflammation, treatment with conventional synthetic (cs) or biological (b) disease-modifying antirheumatic drugs (DMARDs) and the role of other AEs regarding the risk to develop stroke. To address confounding by different risk profiles in patients with and without stroke, we performed a nested case–control study which allowed controlling for known risk factors.
Patients and methods
Data source and assessments
Data of the German biologics register RABBIT (Rheumatoid Arthritis: Observation of Biologic Therapy), a prospective cohort study, were used. Patients with RA are enrolled when starting treatment with a bDMARD or csDMARD after at least one csDMARD failure. Clinical-derived and patient-derived data are reported at predefined time points of follow-up (baseline, at 3 and 6 months, thereafter every 6 months). Regularly collected data comprise disease activity measures, treatment details (eg, start/stop dates of DMARDs and dosages of glucocorticoids) and AEs. Rheumatologists are requested to give additional information about serious AEs (SAEs) and to provide hospital discharge letters.
Comorbidities and whether they were medically treated were reported by the rheumatologists at baseline. Among others, patients specified their physical function (Hannover Functional Status Questionnaire (FFbH)13) and their global health. Further details of RABBIT were reported elsewhere.14–16 The study protocol of RABBIT was approved by the ethics committee of the Charité University Medicine Berlin. Patients have to give their written informed consent prior to enrolment.
Outcome definition
All incident cerebrovascular events reported until 31 October 2015 were reviewed by the study physician of RABBIT (AS). Events were categorised as ischaemic, haemorrhagic and unclassified strokes as well as transient ischaemic attacks (TIAs) and subarachnoid haemorrhages. Only the first event of a non-haemorrhagic stroke (ischaemic or unclassified strokes or TIAs) in a patient was considered in this analysis.
In addition, all reported AEs apart from stroke classified as being serious according to the International Council for Harmonisation (ICH) definition17 with event dates either reported by rheumatologists or from hospital discharge letters were investigated. We categorised the SAEs into: infections, cardiovascular (CV) events but not stroke, surgeries and all remaining SAEs.
Study design: cohort study and nested case–control study
Risk factors for stroke were first analysed with data from the entire cohort. Second, we performed a nested case–control study. Patients who developed a stroke were selected as cases. We applied an extensive matching algorithm with a 1:2 ratio (one case: two controls; they form one cluster). Exact agreement of cases and their controls was required regarding gender, hypertension, coronary heart disease, heart failure, diabetes, smoking habits (never vs ever/unknown) and enrolment episode (2001–2006 and 2007–2015). Age had to be similar in cases and controls (±5 years). Eligible controls had to be under observation at the date of stroke of the matching case (index date).
Definition of treatment exposure
Treatment with DMARDs was categorised into (1) TNF-inhibitors (TNFi) (adalimumab, certolizumab, etanercept, golimumab and infliximab), (2) other bDMARDs (abatacept, anakinra, rituximab and tocilizumab) and (3) csDMARDs. In (1) and (2), a combination with csDMARDs was possible; group (3) was exclusively treated with one or more csDMARD(s). Patients were considered to be exposed to a certain bDMARD up to 3 months after treatment discontinuation (rituximab: 9 months after last infusion).
Current and cumulative treatment was investigated for the use of non-steroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids. The cumulative treatment with NSAIDs was calculated for each patient as the portion of observation time exposed to NSAIDs (range: 0–1). Similarly, cumulative treatment with glucocorticoids was calculated, but additionally weighted for different doses: each month with a dose of >5–10 mg/day was considered with a weight of 0.5 and each month with a dose of >10 mg/day with a weight of 1. The total sum over all weights was divided by the number of follow-up months (range: 0–1).
Patients with hypertension, coronary heart disease, heart failure or hyperlipoproteinaemia but without drug treatment for this condition(s) were labelled as having ‘no CV treatment’. Patients with diabetes or osteoporosis and no treatment were marked accordingly.
Statistical analysis
For baseline comparisons in the cohort study, t-test and χ2 test were applied. In the matched case–control study, univariate linear mixed effects models with a random component for each cluster were used to test for differences between cases and controls.
Risk factors for stroke were investigated using two different approaches: In approach 1, we applied univariate and multiple Cox proportional hazard (PH) models in (1) the whole cohort and (2) the nested case–control study. In the case–control study, we considered the matching structure by the application of a shared frailty Cox regression model,18 which can be interpreted like Cox-PH models (for further explanations see online Supplementary text).
In approach 2, we adapted the idea of multi-state models 19 20 (online Supplementary figure 1). In brief, we were interested in the cumulative incidence of stroke in patients who (1) did not develop or (2) developed an SAE other than cerebrovascular prior to stroke. Exact Poisson confidence intervals were calculated for incidence rates (IRs). Furthermore, we estimated cause-specific hazards to investigate risk factors for stroke in patients without prior SAEs. In this model, patients were censored at the end of the observation (index date) or when other SAEs occurred, whatever came first.
Due to the skewed distribution of CRP values, we used a log-transformation (logCRP) in all models.
Missing data at baseline most frequently concerned smoking status (10.2%), CRP (6.5%), disease activity based on 28 joint count (DAS28) (4.6%) and ESR (3.6%). To analyse the course of disease activity and inflammation, we applied five multiple imputations of missing values. Missing smoking status was coded as a separate category (smoking unknown).
Estimates are shown with 95% CI. Matching was applied using the R-package Optmatch.21 Data were analysed using SAS V.9.4 software.
Results
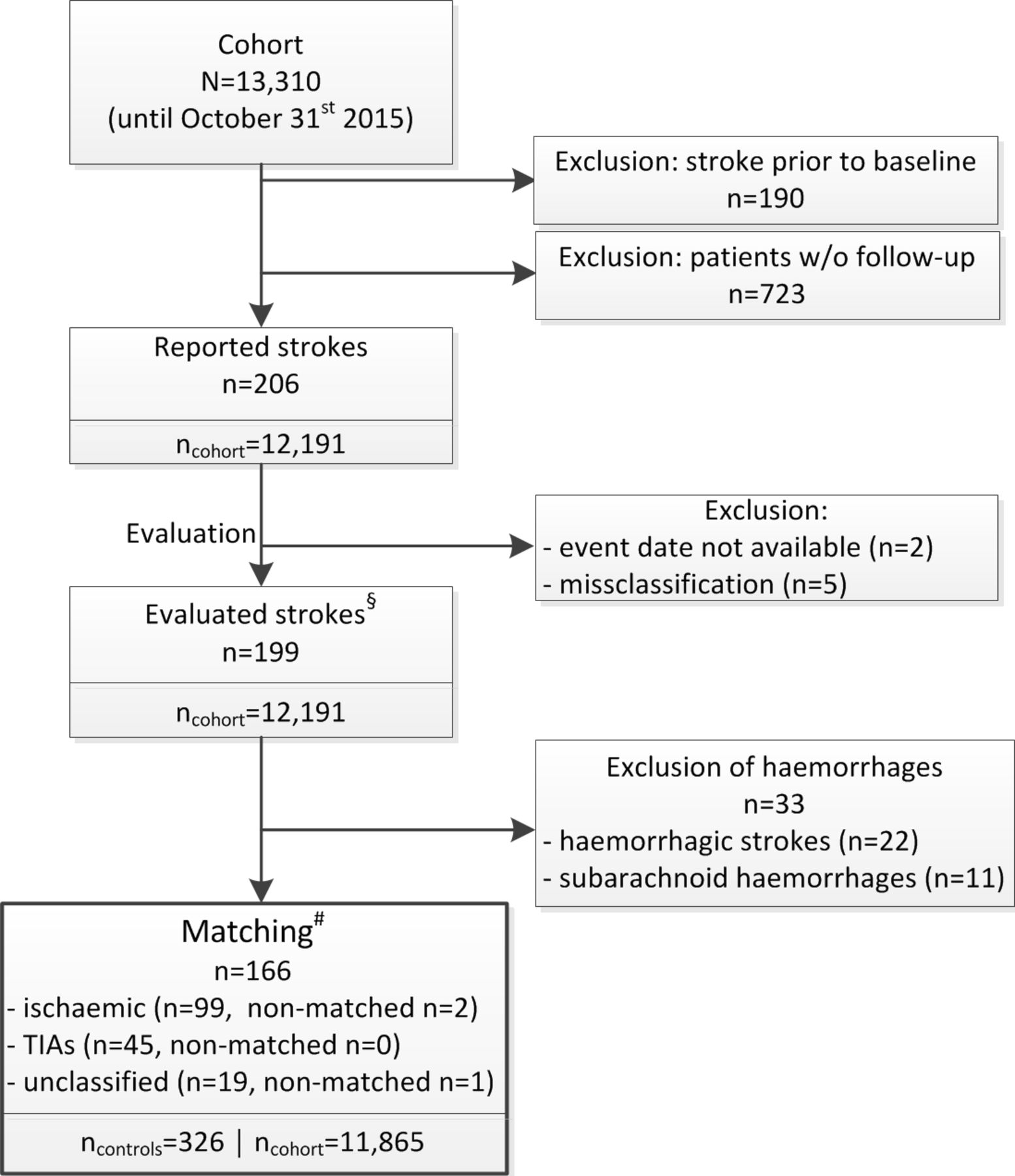
Until 31 October 2015, 206 incident cerebrovascular events were reported (figure 1). We excluded two patients without an available event date and five patients with a misclassification of the reported event. Of 199 events, the majority were ischaemic strokes (n=101, 50.8%), followed by TIAs (n=45, 22.6%), haemorrhagic (n=22, 11.1%) and unclassified strokes (n=20, 10.1%) as well as subarachnoid haemorrhages (n=11, 5.5%). Corresponding baseline characteristics are presented in the online Supplementary table 3. Of the 166 events considered in this analysis (ischaemic strokes, unclassified strokes and TIAs), 163 could be matched to controls (n=326). For one female and two male cases, matching was not possible (online Supplementary table 2).

Flow chart for patient selection and matching. §Diagnoses of evaluated events are listed in the online Supplementary table 1. #Cases were matched to potential controls in a 1:2 manner using the following criteria: gender, age at baseline (±5 years), enrolment episode (2001–2006 and 2007–2015), four baseline comorbidities (hypertension, coronary heart disease, heart failure and diabetes) and smoking habits (never and ever/unknown). Patients with no possible matching are listed in the online Supplementary table 2. TIA, transient ischaemic attack; w/o, without.
Patient characteristics at baseline
Case and control patients were 7 years older than the average cohort patient and differed significantly in comorbid hypertension, diabetes, enrolment period and disease activity at baseline (table 1).
Baseline characteristics of the RABBIT cohort, cases (patients who developed stroke during follow-up) and their matched controls
A significant difference between cases and controls was found regarding the treatment of comorbidities. Of 104 case patients with at least one baseline CV comorbidity, 35 (34%) did not receive CV drug treatment, compared with 21% in controls and in the remaining cohort. Thereof, major gaps were seen regarding hyperlipoproteinaemia (no drug treatment in 78% of cases, 44% of controls and 47% in the cohort) and coronary heart disease (no drug treatment in 40% of cases, 30% of controls and 19% in the cohort). These significant differences in the management of comorbid conditions were not found for diabetes and osteoporosis.
Cumulative incidence of stroke and influences of SAEs in the cohort
The overall rate of incident non-haemorrhagic strokes (n=166) in the RABBIT cohort was 3.2/1000 patient-years (PY) (95% CI 2.7 to 3.7) (online Supplementary figure 2). The IR in patients with no prior SAE was 2.2/1000 PY (95% CI 1.8 to 2.8] and with prior SAE 9.0/1000 PY (95% CI 7.3 to 11.0).
We found a linear increase in the cumulative incidence of stroke in patients who did not experience any SAE prior to stroke (figure 2, left). In contrast, there was an excess risk within the first 30 days after SAEs (figure 2, right). In this interval, the IR was 94.9/1000 PY (95% CI 72.6 to 121.9), dropping significantly to 3.4 (95% CI 2.4 to 4.8) in the period thereafter. Of all reported SAEs, 87.0% led to hospitalisation.

{kind=link}
{kind=link}
Probability of stroke in patients with and without prior SAE. (Left) The probability of stroke after enrolment in patients without any serious adverse event (SAE) prior to stroke; time in days from baseline. (Right) The probability of stroke after SAE; time in days after SAE.
Disease characteristics and treatment of cases, controls and the remaining cohort during follow-up
Patients with stroke presented with significantly higher DAS28 and inflammation markers during the first year of follow-up compared with the remaining cohort in unadjusted analyses. In the nested case–control study, values were insignificantly higher in cases than in controls (table 2). Within 6 months before the event/index date, the mean DAS28 was significantly higher in cases compared with controls.
No differences were observed in the cumulative doses of glucocorticoids, or the use of non-selective NSAIDs and Cox-2 inhibitors.
Disease characteristics in the cohort and in the nested case–control study in different time periods
Risk factors for stroke
In the cohort study, univariate analysis showed a significantly lower risk for stroke in patients with better physical function (FFbH) (table 3). Older age, high values of CRP, ESR and the DAS28 were significantly associated with a higher risk for stroke. Comorbidities such as hypertension, hyperlipoproteinaemia, diabetes, osteoporosis and particularly chronic renal disease were associated with a higher risk for stroke. Except for the current treatment with glucocorticoids, none of the treatments with csDMARDs or bDMARDs, non-selective NSAIDs or Cox-2 inhibitors were associated with the risk for stroke. The highest risk for stroke was found in patients with untreated CV diseases (HR 4.3 (95% CI 2.8 to 6.5)). In the adjusted cohort analysis, only the impact of higher age, physical function and hyperlipoproteinaemia were affirmed. Smoking (ever vs never) was additionally identified as risk factor.
Investigation of risk factors for stroke
In the nested case–control study, univariate analysis showed likewise that high levels of CRP, ESR and DAS28 as well as a poor physical function were significantly associated with a higher risk for stroke (table 3). Significant but smaller effects were found for the comorbidities hyperlipoproteinaemia, chronic renal disease and osteoporosis. Untreated CV comorbidities and the development of SAEs ≤6 months prior to stroke had the strongest association with the risk for stroke. This effect was confirmed in the adjusted shared frailty model with a HR of 3.3 (95% CI 1.5 to 7.2) for untreated CV disease. Regarding SAEs, we found the largest impact for prior serious infections with an HR of 4.4 (1.6 to 12.5). Further significant influences were found for physical function and the number of bDMARD treatments before entering RABBIT. In contrast, current treatment with TNFi, other bDMARDs and glucocorticoids had no association.
To investigate the impact of risk factors in patients without a prior SAE, a cause-specific hazard model was applied (approach 2, table 4). In this model, the associations between physical function as well as untreated CV comorbidities and stroke remained significant. However, the effect size of untreated CV diseases was attenuated to an HR of 2.3 (1.2 to 4.5). The influence of the number of bDMARD treatments before cohort entry was no longer significant.
Cause-specific hazard ratios of stroke in patients without prior SAE
Discussion
We examined the incidence and risk for stroke in a large cohort of patients with RA. The known risk factors age and smoking as well as hyperlipoproteinaemia and a poor physical function were associated with an increased risk. The IR for stroke was highest in patients who experienced another SAE within 30 days prior to stroke. In a nested case–control study with patients at comparable risk for stroke, the absence of CV treatment despite CV comorbidity was associated with a high risk for incident stroke. The highest impact was found for prior serious adverse events, particularly serious infections.
Our results support findings in the general population8 9 and in patients with autoimmune diseases,12 which suggest that stroke may be triggered by other adverse events. Compared with the overall IR of 3.1 strokes per 1000 PY, we observed a high IR of 8.7/1000 PY for patients with a previous adverse event other than cerebrovascular. The association was clearly time-dependent being highest within 30 days (IR: 93.3/1000 PY) after the serious event and dropping thereafter to 3.2. This is in line with results from Smeeth et al who reported an IR ratio (IRR) of 3.2 (95% CI 2.8 to 3.6) during the first 3 days after respiratory tract infections, gradually decreasing in the following weeks.22 Others observed more strokes within 6 days after hospital admission.10 In patients with autoimmune diseases, the risk was highest within 90 days after herpes zoster with an IRR of 1.4 (95% CI 1.1 to 1.7).12
Reasons for the contribution of SAEs to the occurrence of stroke may be diverse. Patients may rest in bed during their illness, with consequences of dehydration and hypercoagulability that can promote embolic events. Previous studies characterised patients with in-hospital onset ischaemic strokes, indicating, among others, fever, high blood pressure, dehydration,10 female gender and atrial fibrillation as risk factors.23
Our data revealed a more than fourfold risk for stroke after serious infections, followed by other SAEs. For CV events, the estimator did not reach statistical significance. Interestingly, surgeries had no effect on the occurrence of stroke (adjusted HR 0.9 (95% CI 0.3 to 2.3)).
Insufficient treatment of CV diseases24 25 and inadequate risk management in RA26 27 were debated widely in recent years. We found that patients who experienced a stroke had been treated less often for their underlying CV diseases compared with control patients or the remaining cohort. This finding is in line with our study on myocardial infarction.28 To preclude a general underreporting of treatment for comorbidity in patients with stroke, we examined the reporting of other comorbidities. Osteoporosis and diabetes were more stringently managed in patients with a future stroke, indicating that awareness for comorbidities differs. However, the guidelines consider the rheumatologist responsible for risk management of CV diseases in RA, in collaboration with cardiologists and other disciplines.29
The treatment with bDMARDs did not influence the occurrence of strokes which is consistent with previous findings.5 30–33 Regarding the effect of glucocorticoids we did not find an association with stroke in the adjusted model and in the nested case–control study. This is in line with previous studies that did not find a negative effect of glucocorticoids on the risk for stroke.5 34 35
Inflammation is discussed as a risk factor for stroke in the general population and in patients with RA,3 6 7 and even considered in the current guidelines for primary stroke prevention of the American Heart Association.36 The association between markers of inflammation and disease activity with the incidence of stroke persisted in our study only in unadjusted analyses. This is in contrast to findings for myocardial infarction.28 However, it implies the possibility of an SAE-driven elevation of inflammation markers. In the cause-specific model, which estimates the risk for stroke without the influence of SAEs, the estimator of logCRP was non-significant (HR 1.1 (95% CI 0.9 to 1.5)) not supporting the idea of CRP as a risk factor for stroke.
Our study has several strengths and limitations. The large RABBIT cohort with well-monitored follow-up data16 enabled us to analyse patients with similar baseline risk for incident stroke, using a nested case–control design. Stroke is a slowly evolving event,37 and controls were required to have a minimum observation time corresponding to their matching case. Requesting the same observation time as matching criteria is a limitation of the study design too, which may imply a selection bias of patients with better controlled disease and less frequent SAEs. This peculiarity may bias the cumulative incidence of strokes after the development of SAEs. Therefore, we omitted this criterion in a sensitivity analysis which confirmed the findings of the main analysis (data not shown). A remaining limitation of shared frailty models rests with the lack of diagnostic tools for evaluation of model assumptions beyond the distribution of random effects.
Conclusion
Aside from traditional risk factors, we found that insufficient CV treatment and the occurrence of other SAEs increased the risk for stroke in patients with RA. These findings, on the one hand, underline the need for rigorous management of CV diseases, on the other hand support results found in the general population which suggest expanding the traditional risk model for stroke by incident other adverse events. This could help to identify patients and clinical situations at increased risk for stroke.
Acknowledgments
The authors acknowledge the invaluable contributions of all participating consultant rheumatologists. In particular, they would like to thank those who enrolled the highest numbers of patients: Kaufmann J, Klopsch T, Krause A, Liebhaber A, Rockwitz K, Eisterhues C, Bergerhausen H, Tony HP, Kaufmann J, Gräßler A, Bussmann A, Burmester G, von Hinüber U, Demary W, Wassenberg S, Kapelle A, Kekow J, Wilden E, Zinke S, Ochs W, Braun J, Richter C, Dockhorn R, Krummel-Lorenz B, Remstedt S, Edelmann E, Schwarze I, Bohl-Bühler M, Berger S, Balzer S, Kellner H, Stille C, Meier L, Aringer M, Tremel H, Bruckner A, Richter C, Röser M, Ständer E, Lebender S, Krüger K, Pick D, Kühne C, Körber H, Fricke-Wagner H, Haas F, Wiesmüller G, Harmuth W, Thiele A, Weiß K, Karberg K, Müller L, Schulze-Koops H, Grünke M, Zänker M, Hamann F, Krause D, Möbius C, Sörensen H, Späthling-Mestekemper S, Dexel T, Alliger K, Schneider M, Schmitt-Haendle M, Manger K, Schuch F, Wendler J, Kleinert S, Iking-Konert C, Moosig F, Grebe T, Seifert A, Menne H, Walter J, Reck A, Gause A, Karger T, Herzer P, Fliedner G, Gauler G, Prothmann U, Häntsch J, Burmester G, Backhaus M, Rech J, Feuchtenberger M, Biewer W, Leumann K, Eidner T, Zeh G, Dahmen G, Riechers E, Schmidt R, Müller-Ladner U, Blank N, Max R, Gause A, Euler H, Möbius E, Winkler K. We also acknowledge the significant contributions of Peter Herzer, Munich, Jörn Kekow, Vogelsang-Gommern, Bernhard Manger, Erlangen and Matthias Schneider, Düsseldorf, as members of the advisory board.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
References
Footnotes
Contributors YM, AR, JL, AZ and AS: had full access to all data of this study and take responsibility for data integrity and accuracy of the analysis. YM, AR, JL, AZ and AS: study concept and design. BM, HPT and EW: acquisition of the data. YM, AR, and AS: analysis and interpretation of the data. YM: drafting the manuscript. YM, AR, BM, HPT, EW, JL, AZ and AS: critical revision of the manuscript for important intellectual content. AZ and AS: obtaining funding. All authors read and approved the manuscript.
Funding RABBIT is supported by a joint, unconditional grant from AbbVie, Bristol-Myers Squibb, Celltrion, MSD Sharp & Dohme, Pfizer, Roche, Samsung Bioepis and UCB. The principal investigators and their team had full academic freedom in study design and conduct, data analysis and publication of results. These stipulations were delineated in their contract with the sponsors. For the purpose of information, all eight funding companies received the manuscript 30 days prior to submission. Publication of this article was not contingent on their approval.
Competing interests YM: no competing interests. AR: honoraria from Pfizer. BM: honoraria for lectures and consulting fees from Abbvie, BMS, MSD, Pfizer, Roche and UCB outside the submitted work. HPT: personal fees from Abbvie, Astra-Zeneca, BMS, Chugai, Janssen, Lilly, MSD, Novartis, Pfizer, Roche and Sanofi outside the submitted work. EW: personal fees from Pfizer outside the submitted work. JL: personal fees from Sandoz and Pfizer outside the submitted work. AZ: grants and personal fees from AbbVie, BMS, MSD, Pfizer, Roche and UCB outside the submitted work. AS: personal fees from BMS, MSD, Pfizer, Roche and Sanofi-Aventis outside the submitted work.
Patient consent Obtained.
Ethics approval The study protocol was approved by the ethics committee of the Charité-Universitätsmedizin Berlin.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data sharing of RABBIT data is not approved.