Article Text

Statistics from Altmetric.com
In a recent meta-analysis, Roberts and coworkers have raised several concerns about the safety profile of paracetamol.1 The criticism was supported by a clear association between exposure and risk of major end points (all-cause mortality, cardiovascular disease (CVD), hypertension, gastrointestinal (GI) disorders, renal failure) and a clear demonstration of a dose–response effect. Although Roberts's message is not conclusive—authors themselves suggest the need of further meta-analyses—it surely has a relevant burden in terms of public health being paracetamol the most largely used drug as first-line therapy for pain disorders.
We present a critical revision of Roberts's meta-analysis following a step-by-step analytical approach.
First, the quality of cohort studies included in the meta-analysis is overtly and intrinsically low.
The authors broadly ascribe the low degree of internal validity of studies collected for the meta-analysis using the GRADE method,2 although this tool is likely unsuitable for quality assessment of non-experimental studies.1
Instead, we adopted the Cochrane A Cochrane Risk Of Bias Assessment Tool (ACROBAT) checklist, which is specifically tailored on observational investigations.3 By doing so, we identified several major methodological pitfalls among the collected studies (table 1).
Risk of bias in observational studies included in Roberts's meta-analysis according to ACROBAT checklist3
Second, most of the discussed examples fail to demonstrate a convincing dose–response effect.
A clear dose–response effect was only revealed for the increased incidence of hypertension estimated by two severely biased studies based on Nurse's Health Study cohort5 ,9 (see the following paragraphs for the details). Notably, Roberts and coworkers support the presence of a dose–response gradient for studies where this relation was instead represented by a plateau (outcome: mortality6); by a U-shaped curve (outcome: mortality,7 GI haemorrhage7); by an ascending trend followed by a clamorous final reverse (outcome: renal failure,8 hypertension9) and by a wavering and/or confusing relations (outcome: myocardial infarction, stroke,7 renal failure7 ,10). In addition, some of these trends—by admission of the same authors6 ,7—were also due to uncorrected confounding bias, namely confounding by indication.
Third, every bias potentially afflicting the paracetamol research is poorly discussed.
We briefly resume our consideration for each individual outcome.
All-cause mortality: Roberts's results likely suffer from confounding bias in particular confounding by indication due to patients' prognosis. Paracetamol tends to be preferentially assigned to sicker and frailer patients, whose prognosis is likely worse; the effect of this confounder is easily explained by temporal trends of mortality rates. In Lipworth's research,6 the standardised mortality ratios peak in the first year of follow-up as well as the crude mortality rates observed by De Vries's.7 In essence, sicker patients assigned to paracetamol died sooner only because of the worse basal prognosis.
Hypertension: Two investigations performed using the Nurse's Health Study cohort4 ,5 represent a classic didactic example of uncorrected detection bias. The outcome was in fact recorded through biennial questionnaires and the diagnosis of hypertension was made by patient's physicians. The pain-affected patients are therefore featured by a greater likelihood to see their doctors, received more prescriptions of analgesics and more diagnoses of hypertension.
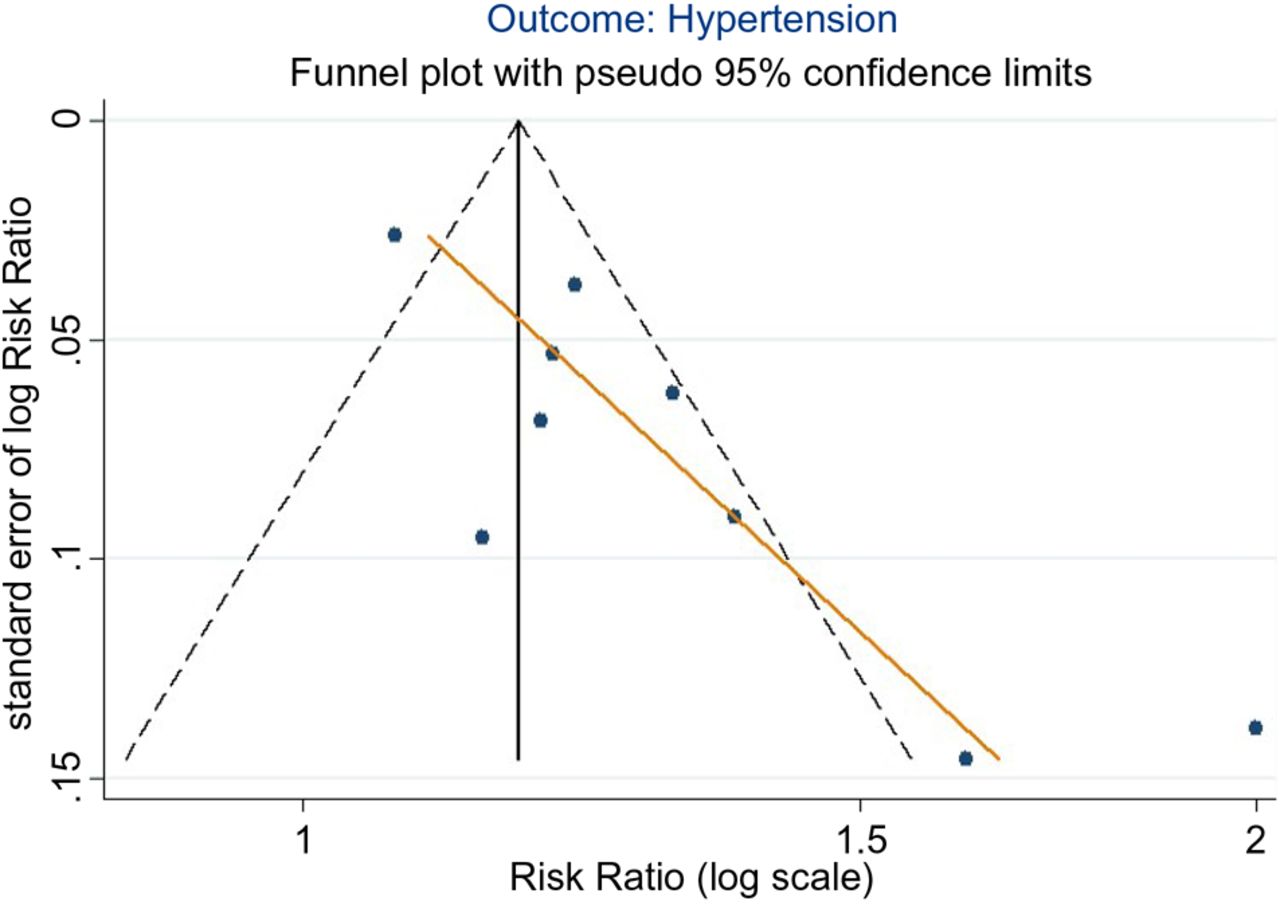
Roberts and coworkers carried out for this end point their unique meta-analytical calculation. Our reanalysis clearly shows the presence of publication bias and/or distortions attributable to biased studies, which have been collected (figure 1). Indeed, both these issues explain the asymmetry of the funnel-plot distribution, which is particularly relevant in the presence of few units of analysis—as is the case—where the statistical power for testing the presence of publication bias is low.2

{kind=link}
Funnel plot—outcome: risk of hypertension. The asymmetry of the risk ratio distribution can be attributed both to serious publication bias (Egger test p=0.006) and to seriously biased results at study level.2
CVD: Chan's research4 was involved into the Nurse's Health Study cohort as well. Non-exposed patients are characterised by a longer duration of follow-up (13 years), whereas the paracetamol users showed a CVD risk proportional to both level of exposure and mean duration of follow-up. In other words, the observation time was stopped in that research: for censoring or for having the outcome at lower and the upper levels of exposure, respectively. Surprisingly, no missing data were reported for the overall 12 years of follow-up.
All data included in Chan's analyses (ie, exposure, outcome, covariates) were collected from last update (ie, from the last biennial questionnaire), so indicating the adjustment was made for variables potentially changed after the exposure to paracetamol. This analytical method is generally not appropriate,3 and authors do not offer sufficient details about it.
CVD end points were also considered by the study of De Vries et al7 : in spite of the lot of covariates used in the regression models, the authors do not adjust for the concomitant use of other analgesics, making the results highly vulnerable to effect of important confounders (eg, use of COX-2 inhibitors). The De Vries study, as admitted by the same author, can be burdened by protopathic bias as well. Namely, the exposure to analgesics may have been justified by symptoms arising right before the diagnosis, being in that manner the outcome antecedent to the exposure.11 Not surprisingly, the risk of myocardial infarction in that study is maximum with the first ever use of paracetamol.
GI end points: This outcome was only studied in the research of De Vries et al7 and surely suffers from confounding by indication due to patients' prognosis. As for mortality, the dose–response relationship was indeed U-shaped. Of note, there were no case–control studies (whose quality was generally better with respect to included cohort studies—data not shown), among those excluded by Roberts's meta-analysis, to show some detrimental effect of paracetamol on GI system.12–17
Renal end points: Two investigations support a kind of kidney damage associated to paracetamol use,7 ,8 while the other two do not.10 ,18 Surprisingly, Roberts supports a detrimental effect for Kurth's results, in overt contrast with the conclusions of the same author (“acetaminophen…does not appear to increase the risk for decline in kidney function”10). This is also the case where observational research on paracetamol might be seriously burdened by confounding by indication, channelling bias and protopathic bias.11 Paracetamol represents generally the first analgesic choice in patients with early signs of renal failure, being in that manner the use of that drug spuriously associable to a greater risk of kidney damage (confounding by indication). At the same time, in the presence of first renal damage, patients earlier exposed to non-steroidal anti-inflammatory drugs (NSAIDs) are frequently shifted to paracetamol use (channelling bias: the use of drugs with similar indications is therefore conditioned by the nature of the end point). Finally, the formerly described protopathic bias can assume in renal disease a particular relevance.11 ,19 On this respect, De Vries reported a bigger risk of acute renal failure for current users of paracetamol in comparison to past users. Furthermore, this study was not adjusted for concomitant use of NSAIDs, which is an important risk factor for acute renal failure.20 ,21 Curhan's research,8 included in the Nurse's Heath Study cohort as well, compared the renal function measured in two blood samples (1989 and 2000) in a small group of nurses (n=1697) whose exposure to paracetamol was retrospectively explored in 1999. Obviously, an initial decline of renal function diagnosed in the range of time between the first and second blood sampling could have been influenced by both confounding by indication and channelling bias, not avoidable by regression adjustment made in that research.
Conclusions
Risk of bias in Roberts's research appears relevant to consent a valid warning about the safety profile of paracetamol, a drug used since 1877 and actually included in the WHO Model List of Essential Medicines.22 Provided that the systematic review of this meta-analysis might be exhaustive, it should be also observed that the quality of available information on this topic is still scarce. Good quality observational studies are therefore needed in attempt to minimise the many types of bias potentially influencing the paracetamol safety research.
References
Footnotes
Contributors All authors fulfil the International Committee of Medical Journal Editors (ICMJE) criteria for authorship credit. AB collected, analysed, interpreted the data, and drafted the manuscript. PLA interpreted the data and edited the manuscript. IC provided management support to research team and edited the article. DF contributed to writing and editing the manuscript. AF contributed to data interpretation and edited the manuscript. CC contributed to data interpretation and edited the manuscript. FL collected and interpreted the data and contributed to writing the manuscript.
Funding This work was supported by the Italian College of General Practitioners and Primary Care.
Competing interests FL and IC provided consultancies in protocol preparation for epidemiological studies and data analyses for IBSA and Angelini. CC and PLA provided clinical consultancies for IBSA, Angelini, Grunenthal, Alfa Wasserman, Pfizer, Prostrakan, Molteni, Dompè and Teva. AF provided clinical consultancies for IBSA. AB and DF have no conflict of interest to disclose.
Provenance and peer review Not commissioned; internally peer reviewed.