Article Text

Abstract
Objectives To explore the effects of tofacitinib—an oral Janus kinase inhibitor for the treatment of rheumatoid arthritis (RA)—with or without methotrexate (MTX), on MRI endpoints in MTX-naive adult patients with early active RA and synovitis in an index wrist or hand.
Methods In this exploratory, phase 2, randomised, double-blind, parallel-group study, patients received tofacitinib 10 mg twice daily + MTX, tofacitinib 10 mg twice daily + placebo (tofacitinib monotherapy), or MTX + placebo (MTX monotherapy), for 1 year. MRI endpoints (Outcome Measures in Rheumatology Clinical Trials RA MRI score (RAMRIS), quantitative RAMRIS (RAMRIQ) and dynamic contrast-enhanced (DCE) MRI) were assessed using a mixed-effect model for repeated measures. Treatment differences with p<0.05 (vs MTX monotherapy) were considered significant.
Results In total, 109 patients were randomised and treated. Treatment differences in RAMRIS bone marrow oedema (BME) at month 6 were −1.55 (90% CI −2.52 to −0.58) for tofacitinib + MTX and −1.74 (−2.72 to −0.76) for tofacitinib monotherapy (both p<0.01 vs MTX monotherapy). Numerical improvements in RAMRIS synovitis at month 3 were −0.63 (−1.58 to 0.31) for tofacitinib + MTX and −0.52 (−1.46 to 0.41) for tofacitinib monotherapy (both p>0.05 vs MTX monotherapy). Treatment differences in RAMRIQ synovitis were statistically significant at month 3, consistent with DCE MRI findings. Less deterioration of RAMRIS and RAMRIQ erosive damage was seen at months 6 and 12 in both tofacitinib groups versus MTX monotherapy.
Conclusions These results provide consistent evidence using three different MRI technologies that tofacitinib treatment leads to early reduction of inflammation and inhibits progression of structural damage.
Trial registration number NCT01164579.
- DMARDs (synthetic)
- Inflammation
- Magnetic Resonance Imaging
- Methotrexate
- Rheumatoid Arthritis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Video abstract
Introduction
Inflammation of the synovium, particularly the bone marrow, measured using MRI, has been identified as a prognostic indicator of structural joint damage in patients with rheumatoid arthritis (RA).1–3 Inhibition of this damage at an early stage in the disease course is desirable to limit disability4 and impact on general health and quality of life.5
Tofacitinib is an oral Janus kinase (JAK) inhibitor for the treatment of RA. The efficacy and safety of tofacitinib 5 and 10 mg twice daily in patients with active moderate-to-severe RA has been demonstrated in randomised, double-blind, phase 26–10 and phase 311–16 studies of up to 24 months duration and in open-label, long-term extension studies with up to 96 months of observation.17 The inhibition of structural damage in patients who received tofacitinib has been shown using plain-film radiography.14 ,15
MRI measures provide improved sensitivity versus conventional radiography.18–20 Bone marrow oedema (BME) and synovitis, measured using MRI, have been shown to be highly sensitive to treatment with conventional synthetic disease-modifying antirheumatic drugs.21–25 However, few randomised clinical trials have been published using MRI outcomes as primary endpoints in patients with early RA.21 ,23 ,26–28 The validated, semiquantitative assessment of multiple pathologies using the Outcome Measures in Rheumatology Clinical Trials (OMERACT) RA MRI score (RAMRIS)29 has become the standard for MRI trials.20 Quantitative MRI measures offer the opportunity to improve on the responsiveness of semiquantitative scoring. Dynamic contrast-enhanced (DCE) MRI measurements show strong correlation with histological assessments of synovitis30 and have demonstrated sensitivity in detecting therapy-induced changes in synovitis in patients with early RA.31 ,32 Preliminary work with active appearance modelling (AAM)33 RA MRI quantification (RAMRIQ) of all involved joint tissues has suggested improved responsiveness over RAMRIS.34
Patients with early RA have participated in previous studies of tofacitinib, although the lowest mean duration of RA was approximately 3 years.14 This is the first study to explore the effects of tofacitinib, as monotherapy or in combination with methotrexate (MTX; vs MTX with placebo), on a range of highly sensitive MRI endpoints, exclusively in patients with early RA.
Methods
Study design and conduct
This was an exploratory, phase 2, randomised, double-blind, double-dummy, parallel-group study (A3921068; NCT01164579), conducted at 24 centres in Central and Latin America, Europe and the USA (25 October 2010–5 November 2013). Study end was the month 12 visit or early termination for patients who discontinued.
Randomisation and treatment
At baseline, patients were randomised 1:1:1 using an automated web/telephone randomisation system to tofacitinib 10 mg twice daily with MTX, tofacitinib 10 mg twice daily with placebo (tofacitinib monotherapy) or MTX with placebo (MTX monotherapy), for 12 months. Tofacitinib 10 mg twice daily was administered orally as two 5 mg tablets twice daily. MTX was administered orally in capsule form and titrated, if tolerated, from 10 mg once weekly (4×2.5 mg capsules) to 15 mg once weekly (6×2.5 mg capsules) at the end of month 1, and 20 mg once weekly (8×2.5 mg capsules) at the end of month 2. Placebo was matched to tofacitinib or MTX, according to randomisation.
Patients
Eligible patients were aged ≥18 years; active RA (>6 tender/painful joints/>6 swollen joints) of ≤2 years duration since diagnosis; erythrocyte sedimentation rate (ESR; Westergren method) >28 mm/h, or C-reactive protein >7 mg/L. Patients were generally MTX-naive, although <3 weekly doses of MTX were permitted after a 4-week washout of MTX, unless MTX had been stopped due to a related adverse event (AE). Key eligibility criteria included unequivocal evidence of ≥1 joint erosion on hand/wrist radiographs (assessed at the study centre), plus clinical evidence of synovitis (tenderness/pain or swelling, or both; confirmed by MRI at the study centre); see online supplementary materials for additional details.
Patients were excluded if they had received prior biological disease-modifying antirheumatic drugs therapy; background arthritis therapy is detailed in the supplementary materials. Other exclusion criteria included replacement of an metacarpophalangeal (MCP) or wrist joint within the index wrist or hand, any contraindications to MRI (glomerular filtration rate <60 mL/min) or previous reaction to gadolinium contrast agent. Patients with malignancies, lymphoproliferative disorder, evidence of untreated latent or active tuberculosis, serious infection ≤6 months previous or infection requiring antimicrobial therapy ≤2 weeks previous were also excluded.
MRI assessments
MRIs were obtained at screening, and at months 1, 3, 6 and 12, using clinical scanners (1.5 or 3.0 T). The same scanner was used serially at any given centre. The contrast agent (0.1 mmol/kg gadolinium) was administered intravenously with an infusion pump. Images included coronal short tau inversion recovery images, pre-contrast and post-contrast coronal T1-weighted (T1w) fat-suppressed gradient echo images, axial DCE T1w gradient echo images and post-contrast axial T1w fat-suppressed spin echo images. Example images are shown in the online supplementary materials.
RAMRIS
MRI BME, synovitis and bone erosions in the index hand (MCP joints 1–5) and wrist were scored according to OMERACT RAMRIS35 by one centralised reader blinded to time sequence and treatment. The presence of any MRI-detected synovitis in the studied joints that were evaluated with RAMRIS (wrist and MCP joints 2–5) was used as MRI confirmation of clinical inclusion.
RAMRIQ
RAMRIQ measurements of BME, synovitis and erosions in the wrist and MCP joints 2–5 were performed by Imorphics (Manchester, UK) using automated methods. RAMRIQ assessed the same pathologies and joints (excepting MCP1) as RAMRIS, allowing for direct comparison of results obtained using the two methods. Bones were automatically identified in pre-contrast, coronal T1 images using AAMs.33 ,36 Joint capsules and soft tissues were also segmented with AAMs, providing consistent 3D regions of interest (ROI) for synovial enhancement across all time points. Oedema volume was defined as non-erosion contrast-enhancing voxels inside the bone. Synovial volume was calculated as voxels that enhance within each ROI. Erosion volume was identified inside the bone surfaces using voxel-based classification. The volume of BME and erosions was normalised to total bone volume for statistical analysis.
DCE MRI
DCE MRI was captured for the wrist only. ROIs were defined by a radiologist within the area encompassing the distal radioulnar joint, the radiocarpal joint and the intercarpal–carpometacarpophalangeal joints. The number of enhancing voxels (NVox), initial rate of enhancement (IRE) and maximum enhancement (EMax),with plateau and washout patterns, were automatically extracted from ROIs and the sum (NVox) or average (IRE and EMax) of values across three user-defined ROIs was determined using the Dynamika software package (Image Analysis, London, UK37).
Endpoints
The co-primary endpoints were change from baseline in RAMRIS BME at month 6, and change from baseline in synovitis at month 3, in wrist and MCP joints.
Changes from baseline in RAMRIS BME (except month 6), synovitis (except month 3) and RAMRIS erosions at months 1, 3, 6 and 12 were assessed as secondary endpoints. Exploratory endpoints included RAMRIQ assessments of BME, synovitis and erosions; DCE MRI assessment of NVox, IRE and EMax; and proportions of patients with/without progression based on RAMRIS BME, synovitis and erosions.
Radiographic and clinical endpoints
Posteroanterior hand/wrist and anteroposterior foot radiographs at baseline, month 6 and month 12, were assessed as secondary endpoints using the van der Heijde modification of the total Sharp score (mTSS)—range 0–488, with higher scores indicating greater structural joint damage.38 Radiographs were scored by a centralised reader blinded to time sequence and treatment received.
Clinical endpoints included American College of Rheumatology (ACR)20, ACR50 and ACR70 responses; proportion of patients achieving a Disease Activity Score (DAS28-4[ESR]) <2.6 (remission) or ≤3.2 (low disease activity); and improvement from baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI) score ≥0.22.
Safety assessments
AEs and clinical laboratory abnormalities were recorded. Medical Dictionary for Regulatory Activities V.16.1 was used.
Statistical analyses
This was an exploratory study. Sample size was determined by change from baseline in RAMRIS BME score at month 6 and RAMRIS synovitis score at month 3. A sample size of 30 patients per arm provided >80% probability to show a statistical difference between arms at the two-sided α of 0.1. Owing to an observed dropout rate of ∼20%, approximately 110 patients were to be enrolled to obtain 90 evaluable patients for the primary endpoint analysis. Given the exploratory nature of the study, statistical significance was assessed at the 10% (two-sided) level. For reporting purposes, treatment differences with p<0.05 (vs MTX monotherapy) were considered significant.
The evaluable set—all patients who were randomised to study treatment, received ≥1 dose of randomised investigational drug and had available data at baseline and the indicated time point—was used for the efficacy analyses.
Primary and secondary continuous efficacy endpoints were assessed using a mixed-effect model for repeated measures, with treatment arms as factors and baseline as a covariate. Categorical endpoints were summarised by frequency (n, %). For efficacy endpoints, 90% CIs were included for the difference in proportions between the treatment arms. Procedures for handling missing MRI values are provided in the online supplementary materials.
Cumulative probability plots examined the distribution of changes from baseline in OMERACT RAMRIS measures and van der Heijde mTSS. The smallest detectable changes (SDCs) for RAMRIS BME, synovitis and bone erosion measurements were determined according to the method described by Bruynesteyn et al39 using month 6 MRI data from 10 patients; read twice by the same reader with >4 weeks between readings to minimise any recall bias. SDCs for RAMRIS BME, synovitis and erosion scores were 1.85, 2.77 and 0.85, respectively.
Results
Patient disposition and demographics
Of 109 patients randomised, 36 received tofacitinib with MTX, 36 received tofacitinib monotherapy and 37 received MTX monotherapy (figure 1). Baseline demographics and disease characteristics were generally well balanced between groups (table 1). Fewer patients who received MTX monotherapy completed the study (58.3% (n=21)) versus those who received tofacitinib with MTX (77.8% (n=28)) or tofacitinib monotherapy (75.0% (n=27)).
Summary of patient demographics and baseline characteristics

Patient disposition. aMean dose of methotrexate (MTX) at month 3 was 18.3 mg weekly; bmean dose of MTX at month 3 was 19.0 mg weekly; ccould not attend scheduled visits due to work. AE, adverse event; BID, twice daily; N, number of patients in population or analysis set; n, number of patients with an event.
Co-primary endpoints
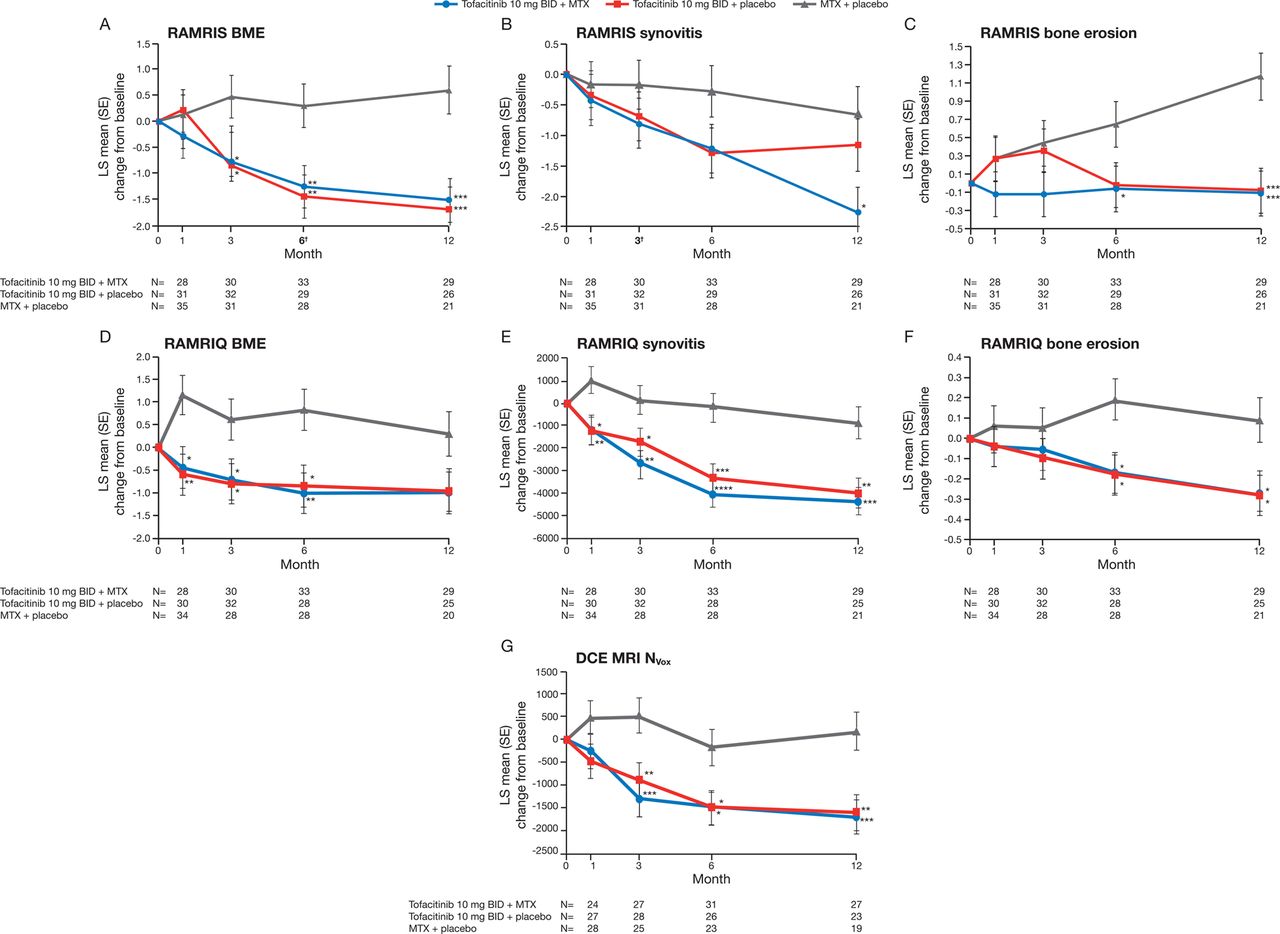
Treatment differences (90% CI) in RAMRIS BME at month 6 were −1.55 (−2.52 to −0.58) for tofacitinib with MTX and −1.74 (−2.72 to −0.76) for tofacitinib monotherapy (both p<0.01 vs MTX monotherapy; figure 2A). Corresponding changes from baseline in RAMRIS synovitis score at month 3 were −0.63 (−1.58 to 0.31; p=0.27) and −0.52 (−1.46 to 0.41; p=0.36) (figure 2B).

Least squares (LS) mean change from baseline in wrist and metacarpophalangeal (MCP): (A) rheumatoid arthritis MRI score (RAMRIS) bone marrow oedema (BME), (B) RAMRIS synovitis, (C) RAMRIS bone erosions, (D) quantitative rheumatoid arthritis MRI score (RAMRIQ) BME, (E) RAMRIQ synovitis, (F) RAMRIQ bone erosions and wrist (G) dynamic contrast-enhanced MRI (DCE MRI) number of enhancing voxels (NVox) (evaluable set). *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001 vs methotrexate (MTX) monotherapy, using a mixed-effect model for repeated measures. MRI measurements were based on one hand (most symptomatic at baseline). RAMRIS and RAMRIQ scores relate to MRIs of the index hand (MCP joints 1–5 and 2–5, respectively) and wrist. DCE MRI measurements relate to MRIs of the index wrist using regions of interest (ROIs) defined within the area encompassing the distal radioulnar joint, the radiocarpal joint and the intercarpal–carpometacarpophalangeal joints. BID, twice daily.
Secondary and exploratory endpoints
RAMRIS
The treatment difference (90% CI) in RAMRIS BME at month 3 was −1.24 (−2.21 to −0.27) for tofacitinib with MTX and −1.32 (−2.28 to −0.37) for tofacitinib monotherapy (both p<0.05 vs MTX monotherapy). Significant differences were maintained to month 12 (figure 2A). Improvements from baseline in RAMRIS synovitis were observed in all groups up to month 12. While improvements were numerically greater in both tofacitinib groups versus MTX monotherapy at all time points assessed, differences were not generally significant (figure 2B). Less deterioration in RAMRIS erosion scores was noted from month 1 onwards in patients receiving tofacitinib with MTX, versus MTX monotherapy (figure 2C). Treatment differences (90% CI) in RAMRIS erosions at month 6 were −0.71 (−1.29 to −0.12) for tofacitinib with MTX (p<0.05 vs MTX) and −0.67 (−1.25 to −0.08) for tofacitinib monotherapy (p=0.06 vs MTX). Corresponding changes at month 12 were −1.29 (−1.90 to −0.69) and −1.26 (−1.87 to −0.65; both p<0.001). Mean values for all RAMRIS measures over time are presented in online supplementary table S1.
Post hoc cumulative probability plots for RAMRIS endpoints
In general, more patients receiving tofacitinib showed regression (ie, improvement <−SDC) in RAMRIS BME (month 6) and synovitis (month 3) versus MTX monotherapy, and a smaller proportion demonstrated progression (ie, deterioration >SDC) (figure 3A,B). The MTX monotherapy group contained a greater proportion of patients with deterioration of erosive damage at month 12 versus both tofacitinib groups (figure 3C). This was mirrored by a smaller proportion of patients with no progression in van der Heijde mTSS (change ≤0.5) at month 12 in the MTX monotherapy group versus either tofacitinib groups (figure 3D).

{kind=link}
{kind=link}
{kind=link}
Cumulative probability plots for rheumatoid arthritis MRI score (RAMRIS) endpoints and van der Heijde modification of the total Sharp score (mTSS). The distribution of changes by percentile is shown. BID, twice daily; BME, bone marrow oedema; MCP, metacarpophalangeal; MTX, methotrexate; SDC, smallest detectable change.
RAMRIQ and DCE MRI
Reductions from baseline in RAMRIQ BME and synovitis were observed for both tofacitinib groups from month 1 to month 12 (figure 2D,E). Treatment differences were significant (p<0.05 vs MTX monotherapy) through month 6 for BME and through month 12 for synovitis (figure 2D,E). Treatment differences in RAMRIQ bone erosion scores showed significantly less deterioration of erosive damage at months 6 and 12 in both tofacitinib groups versus MTX monotherapy (all p<0.05) (figure 2F).
DCE MRI measurements (NVox) indicated significant improvements from baseline in synovitis at month 3 for both tofacitinib groups (p<0.01 vs MTX monotherapy) (figure 2G). Improvements remained significant (p<0.05) through month 12 (figure 2G). Mean values for RAMRIQ and DCE MRI measures over time can be found in online supplementary table S1. Least squares (LS) mean changes from baseline in IRE and EMax are shown in online supplementary figure S1.
Radiographic assessments
Numerical changes from baseline in van der Heijde mTSS, joint space narrowing and erosion component scores were small in all treatment arms at months 6 and 12 (table 2).
Radiographic and clinical endpoints (evaluable set, LOCF)
Clinical response
Numerically higher ACR20, ACR50 and ACR70 response rates were observed at months 3, 6 and 12 in the tofacitinib groups versus MTX monotherapy (table 2). The proportion of patients who achieved DAS28-4(ESR) <2.6 increased over time in both tofacitinib groups, whereas corresponding values in the MTX monotherapy group remained low and stable (table 2). More patients receiving tofacitinib (vs MTX monotherapy) achieved DAS28-4(ESR) ≤3.2 from month 3 onwards (table 2). Compared with MTX monotherapy, the proportion of patients achieving an improvement in HAQ-DI ≥0.22 from baseline in the tofacitinib groups was numerically higher at month 6 and similar at month 12 (table 2).
Safety and tolerability
AEs were reported in 78.9% of patients (86/109), of which 96.1% (245/255) were mild or moderate. AEs are summarised in table 3. Five patients had serious AEs, one of which (anal abscess in a patient receiving tofacitinib with MTX) was considered treatment-related by the investigator, resulted in permanent discontinuation, and was the only serious infection reported. No deaths were reported. Eleven patients discontinued due to AEs (any cause). Liver function test abnormalities were the most common AE that resulted in discontinuation: two patients receiving tofacitinib with MTX, and four patients receiving MTX monotherapy. Six patients receiving MTX monotherapy discontinued due to insufficient clinical response—no tofacitinib-treated patients discontinued for this reason.
Safety events and discontinuations (all causalities)
There were few differences between treatment groups: nine patients (8.3%) had severe AEs, of which eight (7.3%) were randomised to tofacitinib (n=4 in each tofacitinib group); and the proportion of patients with infections (any cause) was higher for tofacitinib with MTX versus the monotherapy groups (table 3).
Discussion
This novel imaging study in patients with early RA provides evidence that tofacitinib 10 mg twice daily, administered as monotherapy or in combination with MTX, can improve MRI outcomes related to tissue inflammation that have been identified as prognostic indicators for joint damage.1 ,40 All MRI methodologies demonstrated reduced inflammation in the synovium and bone marrow with tofacitinib. Numerical trends in semiquantitative and quantitative MRI data were consistent between the two tofacitinib arms. Furthermore, quantitative methodologies identified significant changes in MRI pathologies (inflammation and erosive damage) as early as month 1 or 3, and demonstrated suboptimal treatment-related suppression of inflammation and progressive bone erosions with MTX monotherapy. The study met the first of its co-primary endpoints, with highly significant improvements in RAMRIS BME at month 6 observed for both tofacitinib groups versus MTX monotherapy. Statistically significant improvement in RAMRIS synovitis at month 3 versus MTX monotherapy was not met. However, numerical improvements in RAMRIS synovitis were observed in both tofacitinib groups (vs MTX). Furthermore, significant improvements in synovitis scores were observed over time with tofacitinib when quantitative methodologies were used.
The concordance between results obtained using three different MRI techniques underlines the effectiveness of MRI in the evaluation of joint inflammation and damage. All measures were analysed blind to time order, adding to the robustness of the evaluation. The improved differentiation of tofacitinib groups from MTX monotherapy enabled by the quantitative MRI techniques (compared with the semiquantitative RAMRIS method) further validates their use as improved tools for outcome assessment. RAMRIQ is still in development, and increased responsiveness for bone pathologies is expected.
In this study, changes from baseline in van der Heijde mTSS were small in both tofacitinib groups. This finding, together with the relative proportions of patients with progression in mTSS at month 12 in tofacitinib groups (vs MTX monotherapy), is supportive of the lack of radiographic progression noted in previous studies of tofacitinib as monotherapy, or in combination with MTX, in patients with moderate-to-severe RA.14 ,15 In the present study, trends in radiographic parameters at months 6 and 12 were consistent with MRI data.
The safety and efficacy of tofacitinib was consistent with phase 3 studies of tofacitinib.11–16 No new safety signals were identified in this study.
This was an exploratory study. The RAMRIS SDCs were calculated from intraobserver readings, and this may result in more favourable SDCs than those calculated from interobserver readings. Additionally, the relatively small sample size (<40 patients per group) may have introduced certain limitations. Furthermore, approximately half of the patients randomised to MTX monotherapy failed to complete the study. It is possible that had patients not been lost who were failing on MTX monotherapy, larger treatment differences would have been observed for tofacitinib groups versus MTX monotherapy. However, a separate analysis using last observation carried forward for missing values produced findings that were consistent with those of the evaluable set (not shown).
Conclusions
These results, obtained using a range of highly sensitive MRI endpoints, and incorporating the validated RAMRIS technique and novel quantitative techniques, provide consistent evidence for the benefits of tofacitinib in reducing inflammation in the synovium and bone marrow, and inhibiting progression of structural damage in patients with early RA. The novel, quantitative methods used here may, after further validation, prove more sensitive and discriminating than conventional semiquantitative scoring.
Acknowledgments
The authors would like to thank the study A3921068 investigators, staff and patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors The study was planned and designed by PGC, MØ, JDB, ZX, RZ, BTW, KS and BW. Statistical analyses were planned and executed by RZ. Study data were collected by FI-P, OS-R and PH. Specialist input on interpretation of study data was provided by PGC and MØ (all MRI measures), CW and TF (RAMRIS), MAB (RAMRIQ and DCE MRI) and DvdH (radiography). All authors were involved with drafting and critical evaluation of the manuscript, and approved the final version for submission. All authors meet the criteria for authorship as stipulated in the guidelines of the Uniform Requirements for Manuscripts submitted to Biomedical Journals.
Funding The study was sponsored by Pfizer Inc. Data analysis support was provided by Shirsendu Sarkar and Swati Rizhwani of Sciformix, and was contracted by Pfizer Inc. Medical writing support was provided by Erin Bekes, PhD, and Claire Cridland of Complete Medical Communications, and was funded by Pfizer Inc. Image analysis support for RAMRIQ was provided by Gwenael Guillard PhD of Imorphics Ltd.
Competing interests PGC is on the speaker's bureau of and has acted as a consultant for, AbbVie, Merck, Novartis, Pfizer Inc, Roche and UCB. MØ has received research grants from Abbott/AbbVie, Centocor, Merck and Schering-Plough, and has acted as a consultant for Abbott/AbbVie, Bristol-Myers Squibb, Boehringer-Ingelheim, Eli-Lilly, Centocor, GSK, Hospira, Janssen, Merck, Mundipharma, Novartis, Novo, Orion, Pfizer Inc, Regeneron, Sanofi, Schering-Plough, Roche, Takeda, UCB and Wyeth. MAB is an employee and shareholder of Imorphics Ltd and acted as a paid consultant to Pfizer Inc in connection with analysis of study data. CW and TF are employees of Bioclinica Inc (formerly SYNARC) and acted as paid consultants to Pfizer Inc in connection with analysis of study data. DvdH is a consultant for AbbVie, Amgen, AstraZeneca, Augurex, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Centocor, Chugai, Covagen, Daiichi, Eli Lilly, Galapagos, GlaxoSmithKline, Janssen Biologics, Merck, Novartis, Novo-Nordisk, Otsuka, Pfizer Inc, Roche, Sanofi-Aventis, UCB and Vertex, and is the Director of Imaging Rheumatology BV (not involved in this study). FI-P has received honoraria from Bristol-Myers Squibb, Pfizer Inc, UCB, Janssen and Roche. OS-R has received research grants from AbbVie, Eli Lilly and Pfizer Inc, is on the speaker's bureau of Bristol-Myers Squibb, Genentech, Pfizer Inc and UCB, and is a consultant for Eli Lilly and Genentech. PH has received research grants from, and is a consultant for, Pfizer Inc. At the time of the reported analysis, ZX, RZ, BTW, JDB, KS and BW were all employees and stockholders of Pfizer Inc. BTW is now affiliated to ImaginAb, Inc, Inglewood, California, USA.
Patient consent Obtained.
Ethics approval The study was conducted in compliance with the Declaration of Helsinki, International Conference on Harmonisation Guidelines for Good Clinical Practice and local country regulations. The study protocol and informed consent documentation were approved by the institutional review board or Independent Ethics Committee at each investigational centre.
Provenance and peer review Not commissioned; externally peer reviewed.