Article Text

Statistics from Altmetric.com
Clinically relevant joint destruction has now become infrequent in patients with newly diagnosed rheumatoid arthritis (RA), while other disease outcomes such as functional ability and disease persistence have become more important. Recently, novel auto-antibody reactivities have been identified in RA, with the ultimate aim to better characterise patients with RA. Anticarbamylated protein (anti-CarP) antibodies were recently identified and associated with more severe radiographic progression,1 but the association with other outcomes was unexplored. With great interest we read the study by Humphreys et al,2 reporting more severe functional disability in anti-CarP positive patients with inflammatory polyarthritis. According to the reported unadjusted β-coefficient (95% CI), patients with anti-CarP antibodies had 0.21 (0.14 to 0.29) higher scores on the Health Assessment Questionnaire (HAQ) during a median follow-up duration of 8 years. This association was statistically independent of the presence of anticitrullinated peptide antibodies (ACPA) and rheumatoid factor (RF). In general replication serves to validate occasional findings. Therefore we studied the association between anti-CarP antibodies and the course of functional disability in 1604 patients with RA who were included in two observational cohorts and had 6474 HAQ measurements over time.
A total of 784 patients with RA were included in the Swedish Better Anti-Rheumatic PharmacOTherapy (BARFOT) cohort3 between 1993 and 1999, and 820 patients in the Leiden Early Arthritis Clinic (EAC)4 between 1993 and 2010 (table 1). Both cohorts are described elsewhere.3 ,4 Linear mixed models with HAQ as continuous outcome and anti-CarP status assessed in baseline serum (as described previously)1 as predictor were performed. Adjustments were done for age, gender and initial treatment strategies as described previously.5 To examine if the association was independent of the effects of other auto-antibodies, additional adjustments were made for ACPA and RF status.
Patient characteristics
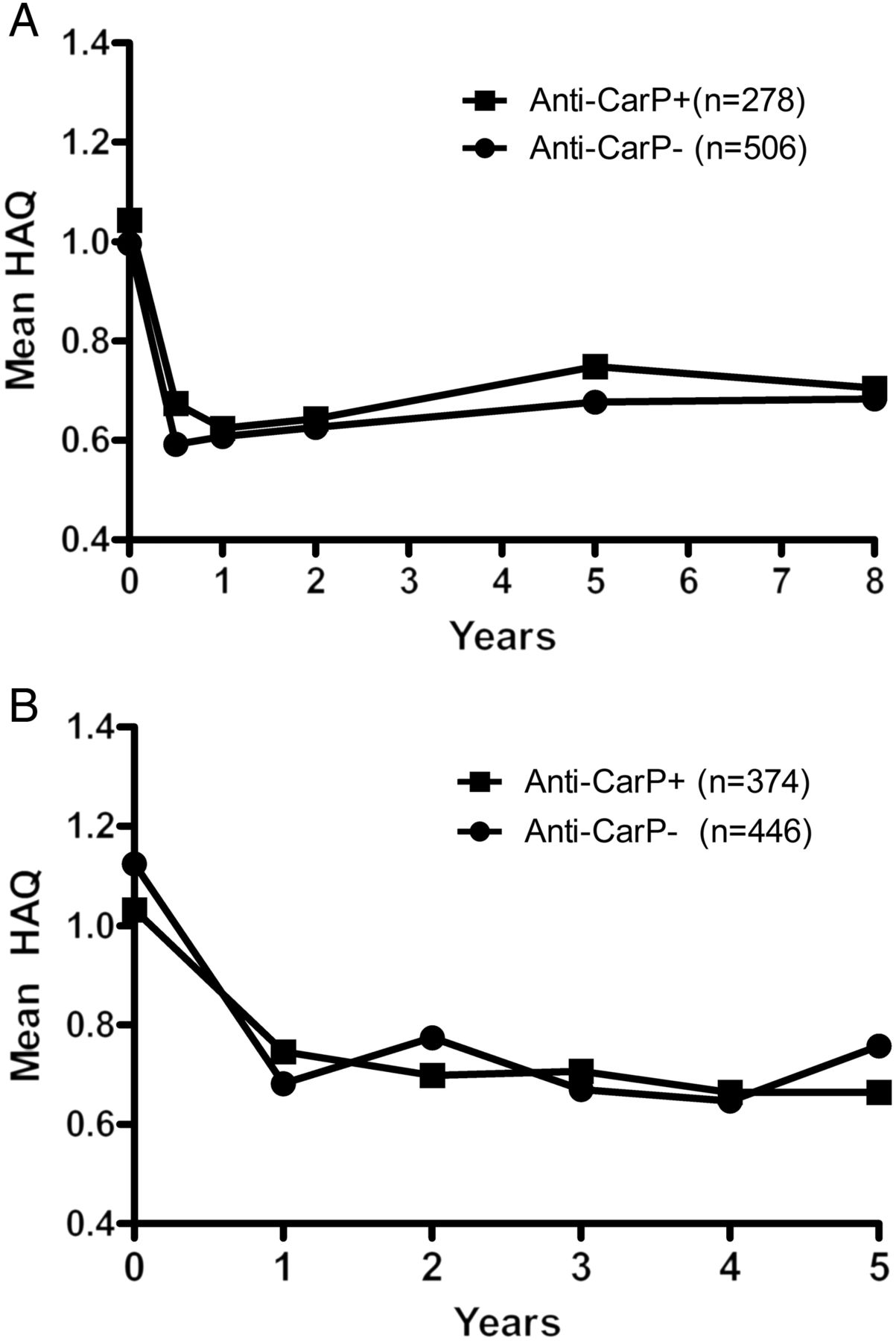
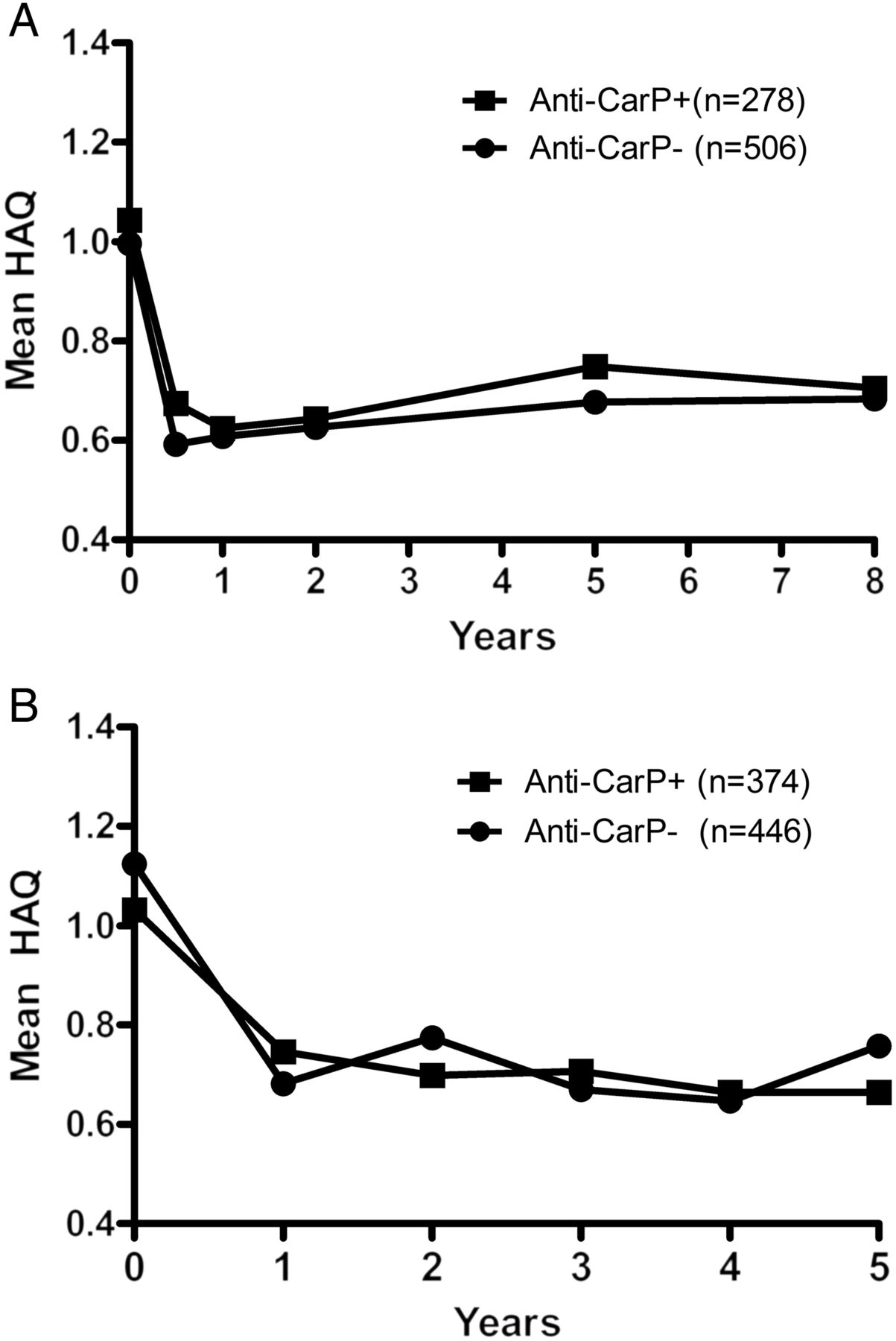
Of the patients with RA, 36% and 46% were positive for anti-CarP antibodies in the BARFOT and Leiden EAC cohorts, respectively (table 1). Univariate analysis within the BARFOT cohort showed that anti-CarP positivity was significantly associated with functional disability; patients carrying anti-CarP antibodies had 0.082 (95% CI 0.0064 to 0.16, p value 0.034) higher HAQ scores during the 8 years of follow-up compared with patients without anti-CarP antibodies (figure 1A). In the model including all three auto-antibodies, anti-CarP was not significantly associated with HAQ over time: effect size of anti-CarP 0.053, 95% CI −0.039 to 0.15, p value 0.26. Also ACPA and RF did not associate with HAQ over time independent of the other auto-antibodies (p values, respectively, 0.29 and 0.94). Within the Leiden EAC, anti-CarP was not associated with functional ability during 5 years of disease: effect size 0.026, 95% CI −0.053 to 0.10, p value 0.52; after additional adjustment for ACPA and RF, the effect size of the association was 0.0051, 95% CI −0.094 to 0.10, p value 0.92 (figure 1B).
{kind=link}
Health Assessment Questionnaire (HAQ) scores during the disease course according to presence of anticarbamylated protein (anti-CarP) antibodies in patients with rheumatoid arthritis (RA) from the (A) Better Anti-Rheumatic PharmacOTherapy (BARFOT) and (B) Leiden Early Arthritis Clinic (EAC) cohorts. Presented are observed mean HAQ scores assessed in (A) 784 patients with RA over 8 years from the BARFOT cohort and in (B) 820 patients with RA over 5 years from the Leiden EAC cohort.
Thus, in contrast to the finding of Humphreys et al, we did not observe that anti-CarP was associated with functional ability, independent of ACPA and RF. Unadjusted analysis in the BARFOT showed an association. However, the effect size of 0.082 was below the minimal clinical important difference (MCID), which is reported to range between 0.09 and 0.38 for the HAQ.6 ,7 Although the effect size observed in the Norfolk Arthritis Register (NOAR) cohort was in this range of MCID, the effects observed in our cohorts were below this limit. In conclusion, we could not replicate that the presence of anti-CarP antibodies is associated with a clinically meaningful difference in functional ability in RA.
Footnotes
Contributors All authors were involved in drafting the manuscript or in revising it critically for important intellectual content. All authors approved the final version to be published.
Funding This work was supported by a Vidi grant of the Netherlands Organisation for Scientific Research, the Dutch Arthritis Foundation, the IMI JU funded project BeTheCure and the Swedish Rheumatism Association.
Competing interests TWJH is on a patent application for the use of anticarbamylated protein antibodies in diagnostics.
Patient consent Obtained.
Ethics approval Local ethics committees.
Provenance and peer review Not commissioned; internally peer reviewed.