Article Text

Abstract
Objectives To examine how comorbid diseases (cardiovascular diseases, hypertension, diabetes, cancer, pulmonary diseases, depression, psychotic disorders and neurodegenerative diseases) affect survival of hip and knee replacements.
Methods Data for this register-based study were collected by combining data from five nationwide health registers. 43 747 primary total hip and 53 007 primary total knee replacements performed for osteoarthritis were included. The independent effects of comorbid diseases on prosthesis survival were analysed using multivariate Cox regression analysis.
Results Occurrence of one or more of the diseases analysed was associated with poorer survival of hip (HR for revision 1.16, 95% CI 1.08 to 1.23) and knee replacements (1.23, 1.16 to 1.30). Cardiovascular diseases and psychotic disorders were associated with increased risk of revision after both hip (1.19, 1.06 to 1.34 and 1.41, 1.04 to 1.91, respectively) and knee replacement (1.29, 1.14 to 1.45 and 1.41, 1.07 to 1.86, respectively). Hypertension and diabetes were associated with early revision (0–5 years after primary operation) after knee replacements (1.14, 1.01 to 1.29 and 1.27, 1.08 to 1.50, respectively). Cancer was associated with poorer survival of hip replacements (1.27, 1.05 to 1.54) and late revision (>5 years) of knee replacements (2.21, 1.31 to 3.74). Depression affected the risk of early revision after hip replacement (1.50, 1.02 to 2.21). Neurodegenerative and pulmonary diseases did not affect prosthesis survival.
Conclusions Comorbid diseases may play an important role in predicting survival of primary hip and knee replacements. The mechanisms underlying these findings and their effect on cost-effectiveness of joint replacements, merit further research.
- Osteoarthritis
- Orthopedic Surgery
- Outcomes research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Joint replacements are safe and cost-effective treatments in late-stage hip and knee osteoarthritis.1 ,2 Currently, <10% of patients require revision surgery over 9–10-years’ follow-up.3–6 Given the high volume of joint replacement surgery and the high cost and sometimes compromised clinical outcome of revisions, patients requiring revision nevertheless constitute a clinically and economically significant minority.7
The indication for surgery, type and fixation of the prosthesis, type of antibiotic prophylaxis and also sex and age contribute to survival of hip and knee replacements,3 ,8–12 whereas the effect of comorbid diseases is not clear. Some studies have ignored comorbid diseases while in others12 ,13 comorbidity has been assessed using proxy measures,14 like the American Society of Anaesthesiologists risk score15 or the Charlson index.16 Although these indices correlate with the surgical outcomes in large series,13 ,14 they have a limited role in guiding the treatment of an individual patient.17 Moreover, relying on comorbidity indices may mask the potentially important specific effects of different diseases. For example, diseases and treatments that impair bone quality might lead to loosening of the prosthesis18 while others, for example, might predispose to infections.19 ,20 On the other hand, comorbidity resulting in decreased physical activity might protect against wear and loosening of the prosthesis.
Use of bisphosphonates has received some attention in earlier literature,21 ,22 and Danish researchers have analysed the effects of diabetes23 and use of diuretics24 and statins25 on survival of hip replacements, but otherwise—to the best of our knowledge—there are no studies on the effects of specific comorbidities on the survival of joint replacements, except for some descriptive case series. The purpose of this study is, therefore, to analyse the effects of several prevalent comorbid diseases with significant clinical and public health importance on survival of primary hip and knee replacements in a nationwide register-based series.
Methods
This study is based on the PERFECT (PERFormance, Effectiveness and Cost of Treatment episodes; http://www.thl.fi/en_US/web/en/project?id=21963) database, maintained by the Finnish National Institute for Health and Welfare. The database was created for continuous monitoring of performance in hip and knee surgery in Finland by combining data from several nationwide health registers. The methodology of the PERFECT project has been described in detail elsewhere.26
Finland has publicly funded healthcare and social insurance. Communities are responsible for providing necessary primary and specialist healthcare services for their citizens, so patients have equal access to healthcare independent of their social or insurance status. Except for emergency cases, referral by a primary healthcare physician (or a private specialist) is required for access to specialist healthcare and is guided by the uniform national criteria for access to elective treatment.
Joint replacement operations
We included primary total hip and total knee replacements performed owing to primary osteoarthritis in 1998 through 2008. The procedures were identified from the Finnish Arthroplasty Register and the Hospital Discharge Register.
The Finnish Arthroplasty Register has collected data on joint replacements since 1980, and since 1997 reporting to the register has been mandatory for orthopaedic surgeons.27 The register includes data on patient demographics, joint operated on, indication for operation and some technical details (for the reporting form, see eg, Puolakka et al27). Compared with the Hospital Discharge Register data, the coverage of primary knee replacements is 96%,28 but accuracy of data has not been scientifically evaluated.
The Hospital Discharge Register is based on mandatory discharge reports. In general, it is considered to be a reliable source of data,29 the accuracy of diagnoses being around 90% or higher.30–32 Coverage of cruciate ligament injuries32 and hip fractures31 exceeds 90%, but the validity of data on joint replacements has not been evaluated. In this study, the included operations were identified based on appropriate diagnosis codes (M16.0, M16.1 M17.0, or M17.1 indicating primary hip and knee osteoarthritis (OA), according to the International Classification of Diseases, 10th revision, as primary diagnosis) accompanied by the surgical procedure code indicating primary total hip or knee replacement (NFB30-60 or NGB20-50 in the Nordic Medico-Statistical Committee classification (http://nomesco-eng.nom-nos.dk/filer/publikationer/NCSP%201_15.pdf)).
In total, 142 488primary hip and knee replacements were identified from the two registers. Of these, 109 555 were primary total hip or knee replacements performed owing to osteoarthritis. Of these, we excluded operations entered in the Hospital Discharge Register but lacking a corresponding record in the Finnish Arthroplasty Register (n=3997; in order to ensure correct linkage of primary and revision operations), operations in patients with a history of conditions suggesting that the aetiology underlying the need for joint replacement was other than primary osteoarthritis (n=8182; see online supplementary text for details), records with missing necessary data (eg, type of joint replacement) in the Finnish Arthroplasty Register (n=2403), operations performed on foreigners or citizens of the autonomous region of Åland Islands (n=566) and simultaneous replacements of a hip and knee on the same patient (n=56).
Comorbid diseases
This study focuses on cardiovascular disease (coronary heart disease, atrial fibrillation and heart failure), hypertension (without concomitant cardiovascular disease), diabetes, cancer, pulmonary disease, depression, psychotic disorders (schizophrenia, schizophrenia-like diseases, mania) and neurodegenerative diseases (Alzheimer's disease, Parkinson's disease, dementia disorders). The effects of coronary heart disease, atrial fibrillation and heart failure were also analysed separately.
Comorbidity data were collected from the Hospital Discharge Register and from the Drug Prescription Register and the Drug Reimbursement Register of the Social Insurance Institution of Finland. Searches of the Hospital Discharge Register were based on diagnosis codes (International Classification of Diseases, 9th and 10th revision), covering all inpatient care in hospitals (both private and public) and primary healthcare wards since 1987.
The Drug Prescription Register includes data on prescriptions supplied by pharmacies since 1994. The Drug Reimbursement Register contains data on patients with certain severe chronic diseases. In Finland, patients with such conditions receive reimbursement (42–100%) for necessary drugs (for details, see http://www.kela.fi/in/internet/english.nsf/ >Sickness >Reimbursements for medical expenses, or Vuorenkoski et al33). Reimbursement is granted based on a medical certificate by the treating doctor. In certain diseases (eg, hypertension) a certificate by a general practitioner suffices, whereas in others evaluation by a specialist is required. The register contains data on reimbursements made since 1964.
Online supplementary table S1 shows the data sources and criteria used to identify the comorbid diseases. In short, hospitalisation data were based on the Hospital Discharge Register, while the drug registers allowed identification of patients with chronic diseases who had not required admission to hospital. A positive record in any of the three registers sufficed for registration of a comorbid condition. Only diseases diagnosed before the operation were taken into account in the analyses.
Follow-up
Revision joint replacements were detected from the records of the Finnish Arthroplasty Register and the Hospital Discharge Register (identified using surgical procedure codes for revision hip and knee replacement) and were linked to corresponding primary operations using Finnish citizens’ unique personal identification numbers and operated joint (hip or knee and laterality). Data on deaths were obtained from the Statistics Finland (http://www.stat.fi/til/ksyyt/index_en.html).
Statistics
The primary outcome was revision joint replacement (removal, exchange or addition of any prosthesis component) for any reason. Patients who had died were censored at the time of death. For the remaining patients, the follow-up ended on 31 December 2009. The minimum follow-up was 1 year unless revision or death occurred before.
Survival of hip and knee replacements (percentage of joint replacements without revision) was calculated using Kaplan–Meier survival analysis and is reported at 1, 3, 5 and 10 years with accompanying 95% CI. The effects of comorbid diseases on survival rates were analysed using Cox regression analysis and are presented as HR with 95% CI.
Cox analysis was first performed in univariate manner for each disease group and then stratified for age (<55, 55–64, 65–74, >74 years) and sex. In these analyses, one disease group was tested at a time. Then, two multivariate models including disease-specific dummy variables (one model with cardiovascular diseases as a single group, the other with cardiovascular diseases split into coronary heart disease, atrial fibrillation and heart failure), age, sex, year of operation, laterality of operation (unilateral, simultaneous bilateral), method of prosthesis fixation and type of operating hospital (university, central, regional or other type of hospital) were run. All diseases were entered simultaneously in the multivariate models to test their independent effects. An additional multivariate model, in which the disease-specific dummies were replaced by a dummy variable ‘any of the diseases’ (occurrence of ≥1 vs none of the diseases), was also run.
Proportional hazards assumption was investigated by testing for a non-zero slope in a generalised linear regression of the scaled Schoenfeld residuals on functions of time in each Cox model.34 If the assumption was not met, the model was run allowing for a step function for the time intervals around the median follow-up (5 years), as suggested by, for example, Ranstam et al.35 This is indicated in the table 2 by separate HRs for 0–5 years and >5 years of follow-up. The multivariate models were performed using a step function for those diseases that did not fulfil the assumption in either univariate or age- and sex-adjusted models.
Finally, the following sensitivity analyses were performed to test the robustness of the multivariate models: (1) inclusion of only cases with fully cemented prosthesis and use of intravenous antibiotic prophylaxis; (2) inclusion of only operations that were patients’ first joint replacements between 1980 and 2010 and (3) use of 3, 4 and 7 years (derived from the survival curves) instead of 5 years as cut-off points in the analyses where the step function was needed for the regression model.
Ethics
The institutional review board of the National Institute for Health and Welfare gave permission for this study. The PERFECT project had previously been approved by the ethics committee of the same institution (THL 1406/6.02.00/2009).
Results
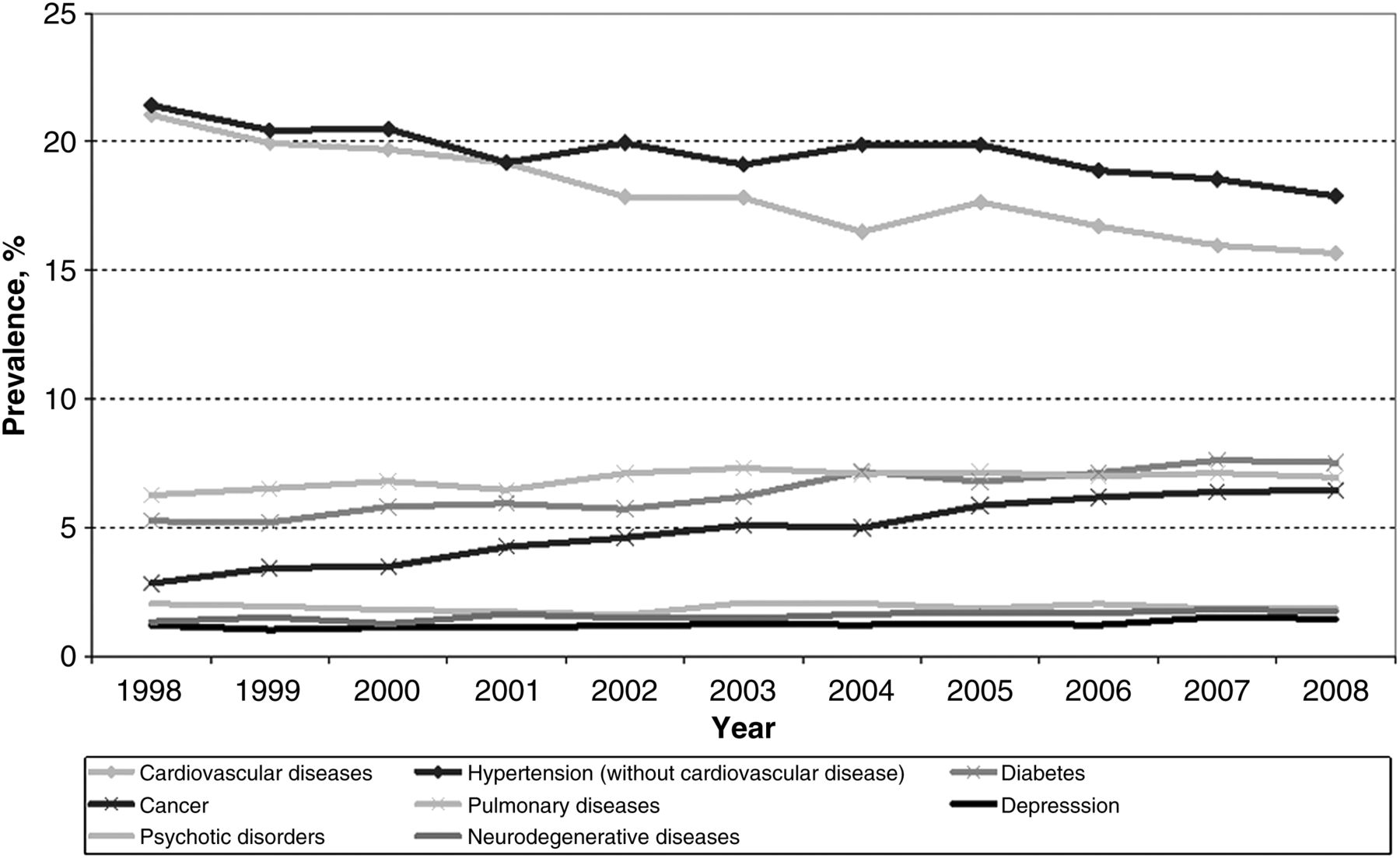
A total of 43 747 primary total hip replacements and 53 007 primary total knee replacements were included in the analyses. Patient demographics, operative data and prevalence of the analysed comorbid diseases are presented in table 1. In general, knee replacement recipients had more comorbidity than hip replacement recipients. During the observation period, the prevalence of cardiovascular diseases declined and the prevalences of diabetes and cancer increased (figure 1).
Patient demographics, prevalence of comorbid diseases and operative data related to primary hip and knee replacements for primary osteoarthritis in Finland from 1998 to 2008
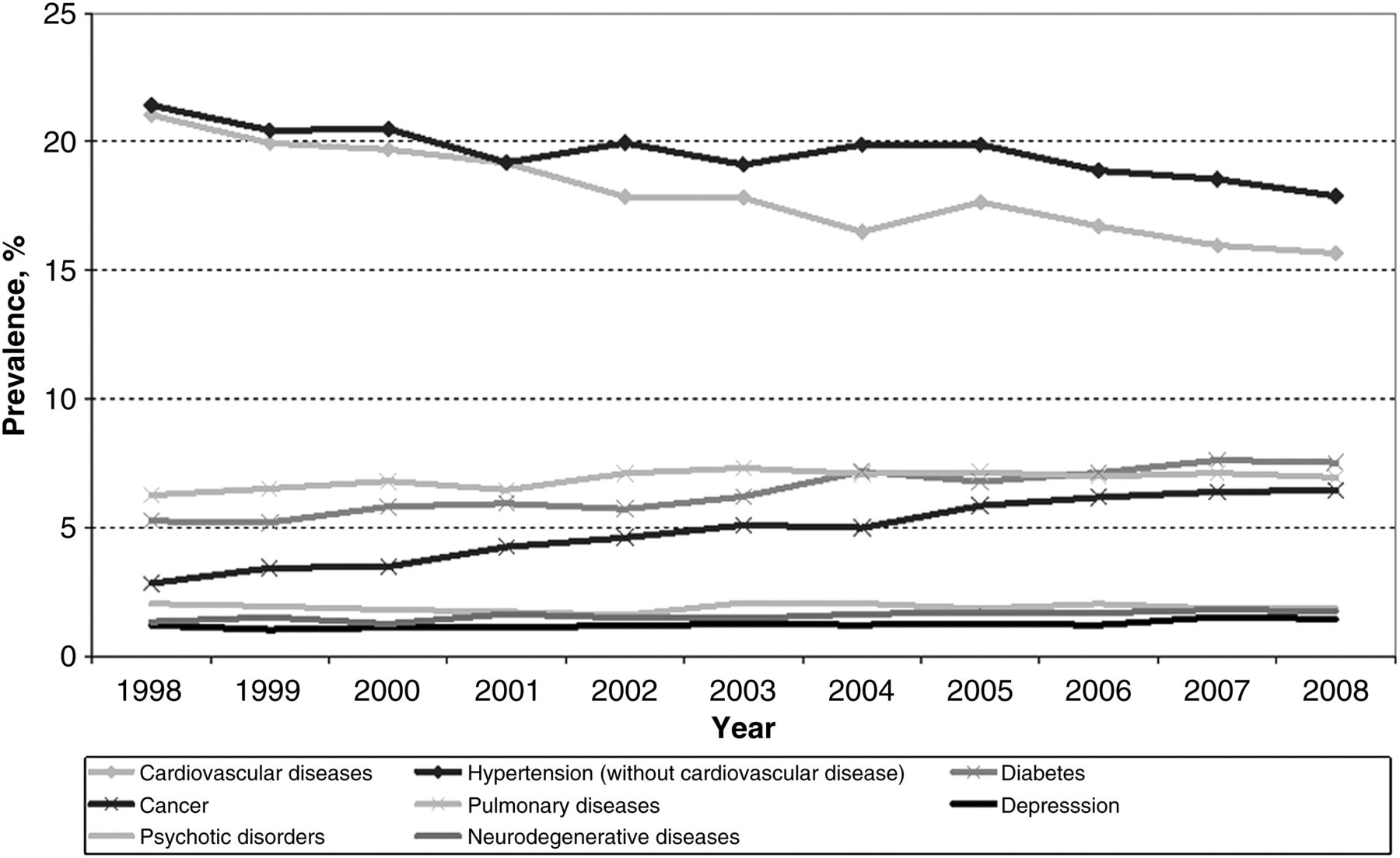
Changes in the prevalence of different comorbid diseases during the observation period from 1998 to 2008 in primary total hip and knee replacements for osteoarthritis.
Prosthesis survival
During the follow-up averaging (median) 4.9 years (range 1–4382 days) after hip replacements and 4.4 years (range 1–4382 days) after knee replacements, 2131 hip and 1919 knee replacements were revised. Death of the patient was the end point of follow-up in 5018/43 747 (11.5%) and 6217/53 007 (11.7%) cases, respectively.
The overall survival rates for hip replacements were 98.8% (95% CI 98.7% to 98.9%) at 1 year, 96.8% (96.7% to 97.0%) at 3 years, 95.7% (95.5% to 95.9%) at 5 years and 91.9% (91.5% to 92.3%) at 10 years. The respective figures for knee replacements were 98.8% (98.7% to 98.9%), 97.1% (97.0% to 97.2%), 96.3% (96.1% to 96.5%) and 94.5% (94.1% to 94.8%).
Survival was poorer in patients with one or more of the diseases analysed both after hip (HR=1.16, 95% CI 1.08 to 1.23) and knee replacements (HR=1.23, 1.16 to 1.30), albeit the differences were slight (figure 2). The effects of separate comorbid diseases on survival of hip and knee replacements are presented in table 2 and the respective survival in online supplementary table S2.
Effect of different comorbid diseases on the risk of revision surgery (calculated using Cox regression analysis) after primary hip and knee replacement

Kaplan–Meier survival curves for prosthesis survival after primary total hip (on the left) and knee replacement (on the right) in patients with and without one or more of the comorbid diseases analysed.
Cardiovascular diseases slightly increased the risk of revision joint replacement (figure 3A). Of the specific conditions, only heart failure was significantly associated with survival of hip replacements, whereas in knee replacements, coronary heart disease, atrial fibrillation and heart failure all independently predicted poorer survival (table 2). Hypertension without concomitant cardiovascular disease increased the risk of early revision knee replacement but had no effect on longer follow-up and in the hip replacements (table 2, figure 3B).

Kaplan–Meier survival curves for prosthesis survival after primary total hip (on the left) and primary total knee replacement (on the right) for osteoarthritis in patients with (A) cardiovascular disease, (B) hypertension (without cardiovascular disease), (C) diabetes or (D) cancer.
Diabetes did not affect survival of hip replacements but was associated with impaired short-term survival after knee replacements (table 2, figure 3C).
A history of cancer was associated with impaired survival throughout follow-up after hip replacement but affected knee replacements only in long-term follow-up (table 2). In the hip replacements, too, the difference became more obvious as follow-up increased (figure 3D).
Although the survival curves indicate slightly lower survival rates in patients with pulmonary diseases than in those without (figure 4A), there was no difference in the multivariate analyses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival curves for prosthesis survival after primary total hip (on the left) and primary total knee replacement (on the right) for osteoarthritis in patients with (A) pulmonary disease, (B) depression, (C) psychotic disorders or (D) neurodegenerative disease.
Patients with depression or psychotic disorders had high revision rates (≥10% at 10 years; figure 4B–C). In the multivariate analyses, depression was associated with early hip prosthesis failure and had no effect in the knee group (table 2). Psychotic disorders instead increased the risk of revision approximately by 40% after both procedures. The effect of neurodegenerative diseases was slighter (figure 4D) and did not reach statistical significance (table 2).
Sensitivity analyses
When only hip replacements with fully cemented fixation and use of intravenous antibiotics were analysed, psychotic disorders and heart failure were no longer associated with survival (HR=0.86, 0.48 to 1.54 and 1.07, 0.77 to 1.47, respectively), whereas atrial fibrillation had a significant effect (HR=1.30, 1.00 to 1.68). Use of different cut-off points for follow-up did not affect the results. Heart failure, coronary heart disease and atrial fibrillation were not significantly associated with survival of first-ever hip and knee replacements, although the direction and the magnitude of the association were similar to the original analysis.
Discussion
Our study showed that comorbid diseases may impair the durability of hip and knee replacements in patients with primary osteoarthritis. The most profound effect was seen for psychotic disorders and depression (figures 3 and 4), although the latter was independently associated only with the risk of early revisions after hip replacements. In general, the revision rates were low and therefore, for example, the increased risks related to comorbidities and differences in survival rates were slight. For several diseases, the 10-year revision rates were approximately 1% higher than in patients without that disease, which corresponds to 10 extra revisions per 1000 operations.
The main strengths of study are the use of a very large and recent series of hip and knee replacements and an almost complete follow-up of all patients. By combining comorbidity data from three different registers, we were able to identify patients managed in outpatient clinics as well as more severe cases who had required admission to hospital and, importantly, we could overcome the usual problem related to poor registration of comorbidities in administrative health registers.
Inevitably, use of register-based data ignores potentially relevant clinical details, which raises a few concerns. First, the effects of obesity and physical activity (that might affect prosthesis wear and loosening) could not be taken into account. Second, we had no data available about the severity of osteoarthritis or that of the comorbid diseases. Patients with poor health are less likely—and also less willing—to undergo joint replacement.36 ,37 It is possible that these patients undergo joint replacement at a later stage of osteoarthritis. However, although poorer preoperative state predicts worse clinical outcome,38 it has not been shown to affect prosthesis survival. On the other hand, high physical activity may predispose the healthiest patients to prosthesis-related failure13 and so level the differences between patients with and without comorbidity. Third, in view of the lack of data about clinical outcome and reasons for revision in different disease groups, the mechanisms underlying our findings remain unclear. Finally, not all data may be 100% correct owing to possible coding errors and, understandably, only diagnosed diseases could be detected from health registers. Nevertheless, it seems unlikely that these factors would have led to systemic bias or to false-positive results. Furthermore, given the low revision rates, it is difficult to collect sufficient clinical material for analyses like ours.
Supporting earlier results,23 diabetes was not associated with compromised overall survival of hip replacements in our study. Nevertheless, diabetes increases the risk of revisions due to deep infection,20 ,23 ,39 which probably explains the high early revision rate of knee replacements in patients with diabetes. The Danish observation about the potentially protective effect of statins25 is in contradiction to the tendency for higher failure rates with coronary heart disease in our study. Earlier observations about higher risk of deep infection and periprosthetic fracture in association with heart failure20 and use of loop diuretics24 again are in line with our results.
Obesity may act as a confounding factor in the analyses concerning cardiovascular diseases and diabetes as it has been associated with greater risk of aseptic loosening.40 In other studies, however, survival rates and occurrence of radiolucent lines around prostheses have been similar in obese and non-obese subjects.41–45 Hence, it is unlikely that obesity alone could have explained our results. The mechanisms explaining how cardiovascular diseases might affect prosthesis survival and the combined effects of cardiovascular diseases and diabetes warrant further research using clinical rather than register-based data.
For other comorbidities, few earlier publications are available. In a recent study,20 heart failure, chronic pulmonary disease, depression, psychoses and metastatic tumours appeared as independent predictors of infection after knee replacement, but prosthesis survival was not analysed. Earlier studies on patients with cancer have been about treatment of bone tumours, whereas in our study, cancer was considered as a comorbid disease, not as an indication for surgery. Impaired long-term survival without many early failures suggests that the difference between patients with and without cancer is due to factors such as prosthesis loosening due to poorer bone quality, but this hypothesis could not be confirmed. Depression predicts prolonged pain and poorer clinical joint scores,46–48 which might explain the relatively high revision rate (figure 4B). On the other hand, the multivariate analyses suggest that the effect of depression largely relates to other comorbidities. We found no studies on the effects of psychotic disorders or neurodegenerative disorders on durability of hip and knee replacements. Against clinical perception, Parkinson's disease and history of stroke did not predispose to hip dislocation in a Scottish study.49
In conclusion, our results should be considered as preliminary evidence indicating that comorbid diseases affect survival of hip and knee replacements. In some disease groups, the effect on survival rates was clinically highly significant, which may impair the cost-effectiveness of joint replacements in affected individuals. The mechanisms of failure and factors predicting the outcomes within the disease groups (like duration of disease and its treatment) warrant further research in order to improve the surgical outcomes in these patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table 1
- Data supplement 3 - Online table 2
Footnotes
-
Handling editor Tore K Kvien
-
Contributors The data used in this study are based on the PERFECT database, maintained and updated by the Centre for Health and Social Economics, Finnish National Institute for Health and Welfare, Helsinki, Finland, which is a governmental agency. MUKL initiated this collaborative project. EJ was responsible for the literature search, drafting of the manuscript and its revisions. MP created the dataset for the study and carried out all statistical analyses. AE and MUKL contributed to the interpretation of the results. All authors contributed to designing the study, interpreting the results and to the important intellectual content of the manuscript. EJ is a guarantor.
-
Competing interests All the authors have completed the unified competing interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no support from any organisation for the submitted work; AE received payment for lectures from DePuy Companies, Stryker Corporation and Biomet, Inc and his institution has received money for travel/accommodation/meeting expenses from DePuy Companies and Biomet, Inc; the other authors have had no financial relationships in the past 3 years with any organisations that might have an interest in the submitted work. There are no other relationships or activities that might appear to have influenced the submitted work.
-
Ethics approval The ethics board of the Finnish National Institute for Health and Welfare (THL 1406/6.02.00/2009).
-
Provenance and peer review Not commissioned; externally peer reviewed.