Article Text

Abstract
Objectives To update the Assessment of SpondyloArthritis international Society (ASAS)-EULAR recommendations for the management of axial spondyloarthritis (axSpA).
Methods Following the EULAR Standardised Operating Procedures, two systematic literature reviews were conducted on non-pharmacological and pharmacological treatment of axSpA. In a task force meeting, the evidence was presented, discussed, and overarching principles and recommendations were updated, followed by voting.
Results Five overarching principles and 15 recommendations with a focus on personalised medicine were agreed: eight remained unchanged from the previous recommendations; three with minor edits on nomenclature; two with relevant updates (#9, 12); two newly formulated (#10, 11). The first five recommendations focus on treatment target and monitoring, non-pharmacological management and non-steroidal anti-inflammatory drugs (NSAIDs) as first-choice pharmacological treatment. Recommendations 6–8 deal with analgesics and discourage long-term glucocorticoids and conventional synthetic disease-modifying antirheumatic drugs (DMARDs) for pure axial involvement. Recommendation 9 describes the indication of biological DMARDs (bDMARDs, that is, tumour necrosis factor inhibitors (TNFi), interleukin-17 inhibitors (IL-17i)) and targeted synthetic DMARDs (tsDMARDs, ie, Janus kinase inhibitors) for patients who have Ankylosing Spondylitis Disease Activity Score ≥2.1 and failed ≥2 NSAIDs and also have either elevated C reactive protein, MRI inflammation of sacroiliac joints or radiographic sacroiliitis. Current practice is to start a TNFi or IL-17i. Recommendation 10 addresses extramusculoskeletal manifestations with TNF monoclonal antibodies preferred for recurrent uveitis or inflammatory bowel disease, and IL-17i for significant psoriasis. Treatment failure should prompt re-evaluation of the diagnosis and consideration of the presence of comorbidities (#11). If active axSpA is confirmed, switching to another b/tsDMARD is recommended (#12). Tapering, rather than immediate discontinuation of a bDMARD, can be considered in patients in sustained remission (#13). The last recommendations (#14, 15) deal with surgery and spinal fractures.
Conclusions The 2022 ASAS-EULAR recommendations provide up-to-date guidance on the management of patients with axSpA.
- Spondyloarthritis
- Biological Therapy
- Therapeutics
Statistics from Altmetric.com
Introduction
Axial spondyloarthritis (axSpA) is a chronic inflammatory rheumatic musculoskeletal disease with a predilection for the axial skeleton. Peripheral (arthritis, enthesitis and dactylitis) and extramusculoskeletal manifestations (EMMs), the latter referring to acute anterior uveitis, inflammatory bowel disease (IBD) and psoriasis, are frequently present.1 axSpA comprises the whole spectrum of patients with and without radiographic sacroiliitis, that is, radiographic axSpA (r-axSpA; also known as ankylosing spondylitis) and non-radiographic axSpA (nr-axSpA), respectively.2–4 Through the years, it has been shown that r-axSpA and nr-axSpA are part of the same disease spectrum and that patients with r-axSpA and nr-axSpA are largely similar with regard to clinical presentation, burden of disease, including the presence of comorbidities, treatment received and response.5–7 Taken together, there is ample evidence to favour the term axSpA, which is why this term has been chosen in these recommendations.8
The management of patients with axSpA includes non-pharmacological and pharmacological interventions. The armamentarium of pharmacological options for axSpA has expanded significantly in recent years. For a long time, if a patient failed non-steroidal anti-inflammatory drugs (NSAIDs), the only alternative options were tumour necrosis factor (TNF) inhibitors (TNFi). Currently, the availability of TNFi, as well as interleukin-17 (IL-17) inhibitors (IL-17i) and Janus kinase (JAK) inhibitors (JAKi), presents more therapeutic options and hope for people living with this disease. Data on the different treatment options come mainly from placebo-controlled trials, with no relevant head-to-head studies performed to date in axSpA. On the other hand, in routine clinical practice, choices between different drugs need to be made throughout the course of patient management. A personalised approach to care, based on individual needs and supported by scientific evidence where available, is crucial. Existing recommendations have tended to show preference for efficacy data along with safety data from observational studies, since these better reflect real-life populations and clinical practice.
Evidence on the efficacy of the different drugs on the EMMs has been accumulating, with data available in patients with pure axSpA or in other populations such as patients with psoriasis, psoriatic arthritis (PsA) or IBD. The efficacy of drugs on EMMs often guides therapeutic choices, hence their value in the management of patients with axSpA. All these aspects underline the importance of regularly updated clinical recommendations that incorporate new evidence to support clinicians in providing optimal management for their patients in daily clinical practice.
The Assessment of SpondyloArthritis international Society (ASAS)-EULAR recommendations for the management of axSpA were first developed in 2006 and updated in 2010, both covering only r-axSpA; then further updated and expanded to the entire axSpA spectrum in 2016.9–11 The current work represents the 2022 update of the ASAS-EULAR recommendations for the management of axSpA guided by the newly available evidence since the 2016 update.
The target users of these recommendations include various stakeholders: (1) all healthcare professionals taking care of patients with axSpA, including not only rheumatologists and health professionals in rheumatology (such as rheumatology nurses or physiotherapists), but also general practitioners, other medical specialists and physicians in training, including medical students; (2) patients with axSpA, to be better informed for optimal shared-decision making; and (3) other stakeholders including patient organisations, regulatory agencies and reimbursement institutions, policymakers, health insurance companies and the pharmaceutical industry.
Methods
The update of the axSpA management recommendations was conducted as a joint project between ASAS and EULAR as per previous years and followed the 2014 EULAR Standardised Operating Procedures (SOPs).12 Following approval by the ASAS Executive Committee and the EULAR Council, the convenors (DvdH, SR) set up a steering committee which included methodologists (EN, AS), fellows (AO, CW) who conducted the systematic literature reviews (SLRs) and two SpA-expert rheumatologists (RBML, XB). Subsequently, the remaining task force members were invited, making a total of 33 participants, from 16 countries across Europe and North America. The current task force consisted of 52% new members compared with the 2016 task force. The 2022 task force membership included rheumatologists, epidemiologists, EULAR representatives from the health professionals committee, People with Arthritis/Rheumatism across Europe, EMerging EUlar NETwork and Young-ASAS. Additionally, five members were recruited through an open call to EULAR countries via a competitive application process. As required by the EULAR SOP, all members disclosed their conflicts of interest upfront.12
The steering committee defined the research questions of the SLRs. Under the guidance of the methodologists, two fellows performed two SLRs: one focused on non-pharmacological and non-biological pharmacological treatment (AO), the second addressed biological disease-modifying antirheumatic drugs (bDMARDs) (CW). These SLRs included studies published from the end search date of the previous SLRs (ie, 2016) up until 1 January 2022, and are published separately.13 14 The SLRs and the current recommendations manuscript form an integral and inseparable part and should be read as such. The results of the SLRs were discussed with the steering committee, which prepared the first draft of the update of the overarching principles (OAPs) and recommendations. The 2016 recommendations were used as a basis, to facilitate the start of the discussion with the complete task force. The basic rule was that a change would only be made if new evidence mandated it.
At the task force’s 1-day online meeting in February 2022, the SLRs were first presented, and their findings discussed. The evidence collected in the previous SLRs was also taken into account and summarised to the entire task force.15–19 In addition to the evidence from the SLRs, expert opinion was considered when formulating OAPs and recommendations. Efficacy and safety, as well as cost-related aspects of interventions, were considered. Costs were considered particularly relevant when different therapies presented similar efficacy and safety, as expensive drugs impose an important burden on healthcare budgets. The usual terminology for DMARDs has also been applied here: conventional synthetic (cs)DMARDs for drugs such as sulfasalazine and methotrexate; bDMARDs for drugs such as TNFi and IL-17i and targeted synthetic (ts)DMARDs for JAKi.20
Recommendations were edited live according to the comments made, followed by a formal voting using anonymised polls. Consensus was reached if ≥75% of the members voted in favour of the recommendations in the first (or ≥67% and ≥50% in a second and third) round. If multiple rounds of voting were necessary, discussion took place in between voting rounds to refine the drafted statements.
After the meeting, the levels of evidence (LoE) and grades of recommendation (GoR) derived from the SLRs following the standards of the Oxford Center for Evidence Based Medicine were added by the steering committee to each of the recommendations.21 Finally, each task force member anonymously indicated their level of agreement (LoA) through an online survey (numerical rating scale ranging from 0=‘do not agree at all’ to 10=‘fully agree’). The mean and SD of the LoA as well as the percentage of agreement ≥8 were presented.
Based on identified gaps in evidence, a research agenda was formulated. The draft of the manuscript was sent to all task force members for review. The final manuscript was approved by all authors, the ASAS Executive Committee and the EULAR Council.
Results
Overarching principles
As commonly seen, OAPs precede the recommendations to indicate a set of crucial principles in the treatment of axSpA, reflecting state-of-the-art management (table 1). Five OAPs were agreed and unchanged compared with the 2016 update.
ASAS-EULAR recommendations for the management of axSpA, 2022 update
A. axSpA is a potentially severe disease with diverse manifestations, usually requiring multidisciplinary management coordinated by the rheumatologist
This OAP underlines two important aspects. First, that musculoskeletal and extra-musculoskeletal manifestations of axSpA often have an important impact on the patient’s life.22 Second, that the rheumatologist, as the expert across the spectrum of the disease, should coordinate the multidisciplinary management. Other medical specialists as well as health professionals may have relevant contributions to the management of patients with axSpA.
B. The primary goal of treating the patient with axSpA is to maximise long-term health-related quality of life through control of symptoms and inflammation, prevention of progressive structural damage, and preservation/normalisation of function and social participation
Management should be aimed at obtaining the best possible health-related quality of life (HRQoL). One way to achieve this is to intervene on disease domains that ultimately impact on HRQoL, namely disease activity, structural damage and function as demonstrated in a stratified model for health outcomes in axSpA.23 24 As axSpA is an inflammatory disease, with most available treatments aimed at reducing inflammatory burden, the control of inflammation has a prominent place in its management, given the impact of disease activity on structural damage and function.25–27
C. The optimal management of patients with axSpA requires a combination of non-pharmacological and pharmacological treatment modalities
This OAP applies to several, and likely all, rheumatic and musculoskeletal diseases. Nevertheless, the combination of both treatment modalities is particularly relevant in axSpA and none should be neglected.14 19 Non-pharmacological treatment is integral to optimal axSpA management.
D. Treatment of axSpA should aim at the best care and must be based on a shared decision between the patient and the rheumatologist
Each individual patient should get the best possible care, preferably tailored to their situation. The decision on the best care for an individual patient has to be taken after careful and informative dialogue between the patient and the healthcare provider (‘shared decision’). As such, this OAP is generic, and can be found in several EULAR management recommendations.28 Shared decision-making is formally defined as a collaborative process between patients and healthcare providers, whereby care decisions are agreed and based on the best scientific evidence available, the health professional’s experience, as well as the patient’s values and preferences.29 Shared decision-making is strongly supported by organisations such as ASAS and EULAR as an essential component of the patient’s care plan.
E. axSpA incurs high individual, medical and societal costs, all of which should be considered in its management by the treating rheumatologist
It is crucial to keep the high costs associated with axSpA in mind, in the broader sense, while trying to achieve the best possible balance in the management of the patient. For the individual patient, the disease represents suffering and burden of disease, with adverse effects on work productivity and consequently economic burden, to the person living with the disease as well family members. Societal costs are mainly driven by healthcare costs and by impaired work productivity with presenteeism, sick leave and work disability, all of them contributing to the economic burden.30 Expensive modern drugs substantially contribute to healthcare costs. Rheumatologists have thus additional societal, as well as individual responsibility for considering costs when making treatment decisions, particularly since more efficient allocation of limited resources will allow the treatment of more patients.31 Notwithstanding, this OAP must not contradict the previous one, which implies that cost considerations cannot over-rule the best care for the individual patient. Combining both principles, deliberately presented in this order, means that when a choice needs to be made between two drugs with comparable efficacy and safety, then the one with the lowest cost is preferable. This principle was also taken into account when formulating the recommendations.
Recommendations
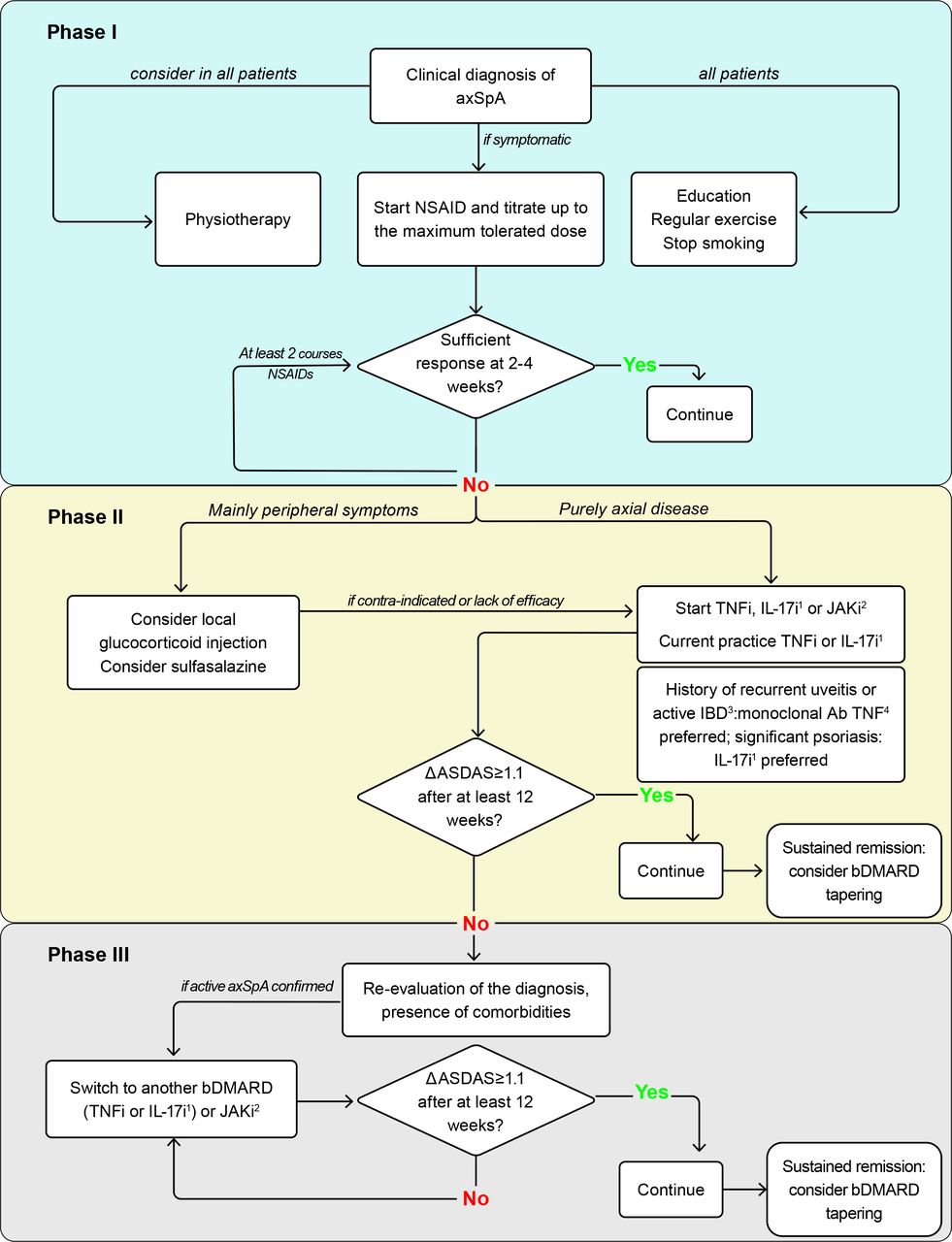
Fifteen recommendations were agreed: eight remained unchanged from the previous recommendations (#2, 3, 6, 7, 8, 13, 14, 15), three received minor edits, mostly on nomenclature (#1, 4, 5), two were significantly updated (#9, 12), while two were newly formulated (#10, 11). Table 1 displays all recommendations, with their corresponding LoE, GoR and LoA. LoA was very high, around or above 9. Figure 1 depicts the algorithm summarising the recommendations, which requires the explanatory text below.
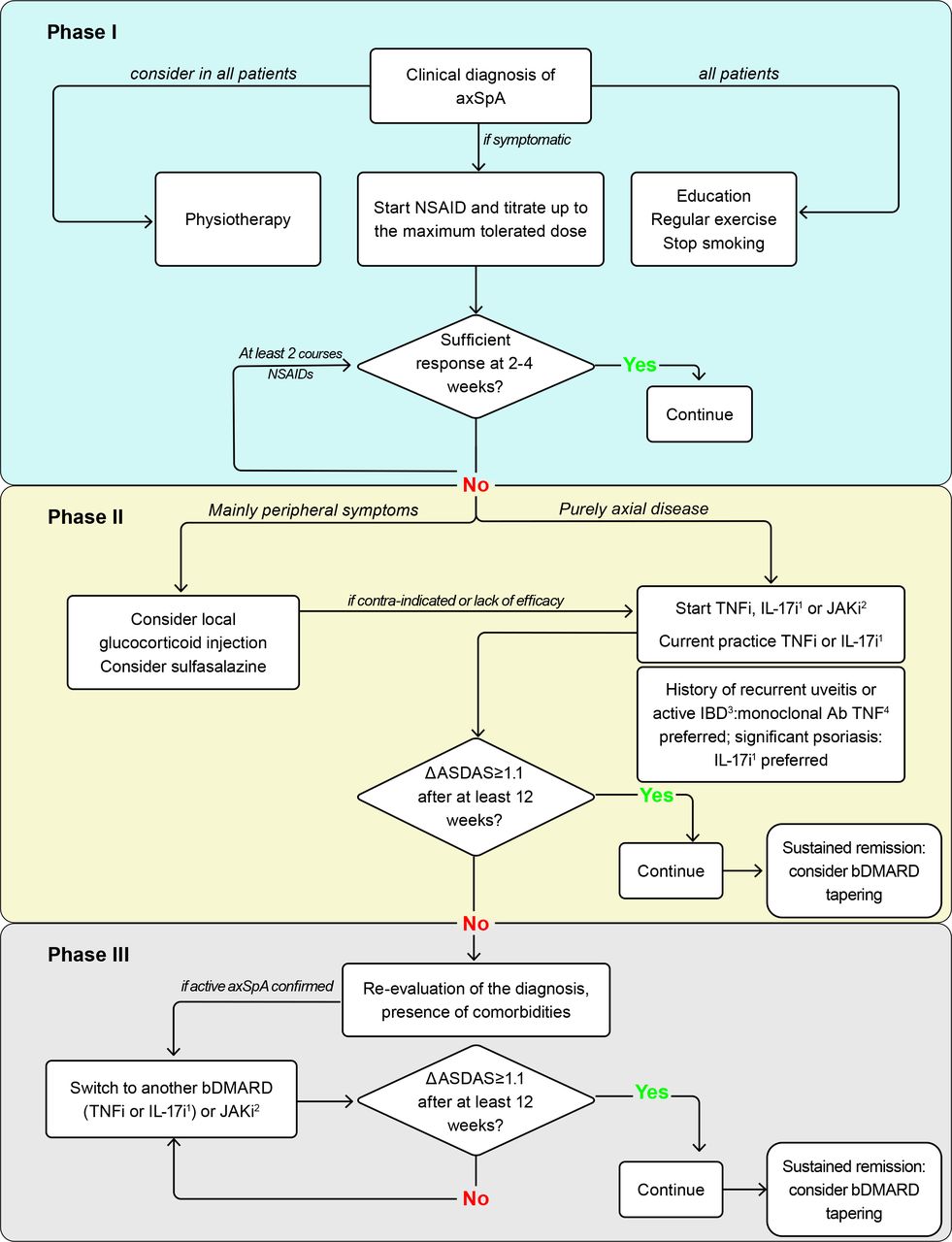
Algorithm based on the ASAS-EULAR recommendations for the management of axial spondyloarthritis (axSpA). Ab, antibody; ASAS, Assessment of SpondyloArthritis international Society; ASDAS, Ankylosing Spondylitis Disease Activity Score; bDMARD, biological disease-modifying antirheumatic drug; IBD, inflammatory bowel disease; IL-17i, interleukin-17 inhibitors; JAKi, Janus kinase inhibitors; NSAID, non-steroidal anti-inflammatory drug; TNFi, tumour necrosis factor inhibitors.
Recommendation 1
The treatment of patients with axSpA should be individualised according to the current signs and symptoms of the disease (axial, peripheral, EMMs) and the patient characteristics including comorbidities and psychosocial factors.
AxSpA has a heterogeneous presentation, and individual disease characteristics and patient needs necessitate a personalised approach to care with shared decision-making at its core. Particularly, when making treatment decisions, the rheumatologist needs to be informed on the presence as well as the extent of the different SpA manifestations, namely axial, peripheral and EMMs. Compared with the previous recommendations, only a minor edit was made to reflect the update of the nomenclature, as EMMs is the currently used term to refer to uveitis, psoriasis and IBD.32 The recommendation intentionally mentions comorbidities due to their impact on disease assessment, outcomes and treatment.33
The task force considered important to emphasise, first and foremost, that a diagnosis of axSpA should be made or confirmed by a rheumatologist (figure 1). A clinical diagnosis of axSpA, based on the clinical presentation, in combination with laboratory and imaging tests, and excluding other potentially more likely diagnoses, is the starting point and should not be based on classification criteria (eg, ASAS axSpA classification criteria). Fulfilment of classification criteria is used for research purposes, to include a homogeneous patient population in a study, but falls short for diagnosis.
Recommendation 2
Disease monitoring of patients with axSpA should include patient-reported outcomes (PROs), clinical findings, laboratory tests and imaging, all with the appropriate instruments and relevant to the clinical presentation. The frequency of monitoring should be decided on an individual basis depending on symptoms, severity and treatment.
Disease monitoring should reflect the different manifestations of the disease and the core domains that have been selected by experts and patients as being the most important. Although these core domains are selected for use in clinical trials, they indicate what patients and rheumatologists consider important.23 32 As an inflammatory disease, monitoring disease activity is crucial in axSpA. In the last decade, the Ankylosing Spondylitis Disease Activity Score (ASDAS) has emerged as the most appropriate instrument for the assessment of disease activity, being recommended when monitoring patients with axSpA.32 34 ASDAS, preferably calculated using C reactive protein (CRP), is a well-balanced index without redundancy across its items, in contrast to the historically more widely used Bath Ankylosing Spondylitis Disease Activity Index (BASDAI).35 Moreover, ASDAS incorporates the perspective of the patient and includes CRP as an objective measure of inflammation while the BASDAI reflects only the patient perspective.35 36 ASDAS has also been validated with a quick-quantitative CRP assay, further improving its feasibility for daily clinical practice.37 38 ASDAS has been shown to be longitudinally associated with syndesmophyte formation.25 27 39 BASDAI alone was not associated with damage progression, except when combined with CRP and with a weaker relationship compared with ASDAS.25 Specific cut-offs have been validated for the ASDAS to define disease activity states and improvement and worsening criteria.40 41 Furthermore, the ASAS core set for monitoring in clinical practice remains an important guide.42 This includes questionnaires collecting PROs for levels of pain, fatigue, morning stiffness and physical function (Bath Ankylosing Spondylitis Functional Index), as well as swollen joint counts, spinal mobility and assessment of EMMs.42 43 A more recently developed instrument, the ASAS Health Index (ASAS-HI), is disease specific and measures overall functioning and health.44 In the context of several PROs used in the monitoring of axSpA, remote monitoring or e-health, with the use of apps or PROs imported into electronic medical records, can contribute to a more comprehensive assessment of the patient to inform further treatment decisions.45 46 Also in line with the ASAS Quality Standards, the task force recommends comprehensive assessments of the patient, including an initial assessment and a comprehensive annual review.47 This is meant to ensure a holistic approach to the patient and that all aspects of the disease are under control, aiming at achieving the treatment goal (OAP 2). Following OAP 1, such assessments should be performed by a multidisciplinary team coordinated by the rheumatologist.
MRI of the sacroiliac joints (SIJ, MRI-SIJ) or of the spine can assess axial inflammation. However, the association between clinical disease activity measures and MRI inflammation is only modest.48–50 MRI is not routinely recommended for monitoring, as its value for this purpose is still unclear and its frequent use is considered unfeasible due to the high costs. Nevertheless, when in doubt about the origin of complaints or about the presence of inflammatory activity, MRI can assist in determining whether inflammation is present and thereby guide the therapeutic decision.
Structural damage can be assessed with radiographs of the spine and the presence of syndesmophytes has a prognostic value, as it reflects higher risk for the development of more syndesmophytes.25 27 51 52 However, structural damage progression occurs at a slow rate and therefore subsequent radiographs of the spine, if performed, should have at least 2-year intervals.51 53
Recommendation 3
Treatment should be guided according to a predefined treatment target.
Treatment towards a predefined target, agreed upon via shared decision between patient and rheumatologist, has been increasingly used in the area of inflammatory arthritis. In axSpA, evidence has only more recently emerged that a higher ASDAS leads to more syndesmophyte formation, which makes ASDAS an appropriate target.25 27 Subsequently, one treat-to-target (T2T) trial has been conducted, TICOSPA, showing that T2T with ASDAS <2.1 as the target is not significantly superior to usual care in achieving an improvement in the ASAS-HI ≥30%, the primary endpoint of that trial.54 While formally a negative trial, T2T showed some efficacy on secondary outcomes. Altogether, the real effectiveness of T2T in axSpA remains undetermined. Therefore, the task force emphasised that a treatment target should be used as a guidance, but should only result in intensifying immunosuppressive treatment if physician and patient are convinced of the presence of residual inflammatory activity and other (contextual) factors do not impede such an intensification. These include aspects that can potentially influence the assessment of disease activity, such as fibromyalgia and other comorbidities.
Recommendation 4
Patients should be educated about axSpA and encouraged to exercise on a regular basis and stop smoking; physiotherapy should be considered.
This recommendation focuses on non-pharmacological treatment, which in axSpA is of prime importance (figure 1).55 All patients should receive education about the disease, as the starting point of self-management, to empower and involve them as active partners in their care.28 56 Patient education in broader terms should include information on the disease, its symptoms and recognition, disease course, treatment options and prognosis.
Exercise is a cornerstone in the management of axSpA, with demonstrated benefits on disease outcomes independent of pharmacological treatment.14 57 While exercise in general should always be part of the disease management, evidence from qualitative studies shows that adherence is higher if supervised.14 Physiotherapy, specifically supervised exercise, has also proven to be more efficacious than home exercises.58 Of note, the heterogeneity and methodological limitations across studies on exercise and physiotherapy hamper a definitive conclusion regarding which exercises are best to perform.14 On an individual basis, physiotherapy should be considered, especially if a patient does not exercise on their own. The task force underlined that physiotherapy should not be an umbrella term also used for interventions that are not widely tested or have proven benefit, like needle knife or complementary medicine-derived practices.14 59 60 After discussion, the task force concluded that ‘physiotherapy’ is a more appropriate term than ‘physical therapy’ as used in the previous version of the recommendations and therefore this small change was incorporated.
Smoking has been shown as a risk factor for spinal inflammation and disease progression in axSpA.61–65 Though no formal investigation has been conducted on the benefits of smoking cessation on axSpA outcomes, it seemed reasonable to recommend it, on the basis of all well-known health risks associated with smoking.
Recommendation 5
Patients suffering from pain and stiffness should use an NSAID as first-line drug treatment up to the maximum dose, taking risks and benefits into account. For patients who respond well to NSAIDs, continuous use is preferred if needed to control symptoms.
NSAIDs are the first line of the pharmacological treatment in axSpA (figure 1). By suppressing inflammation, NSAIDs often suffice in keeping disease activity and symptoms under control.66 This recommendation only has a minor textual change in its last part, which was considered to convey the message more clearly. The task force supports using continuous NSAIDs above on-demand only if needed to control symptoms. Whenever continuous use is not needed to control symptoms, preference should be given to on-demand NSAID treatment, given the risks of long-term use. Historically, this recommendation has also been discussed in light of the contradictory evidence on the effect of NSAIDs on the inhibition of structural damage progression.67–70 The task force hereby emphasises that, to date, the decision on the continuous use of NSAIDs should be based solely on the control of symptoms and not on any attempt to control structural disease progression.
Recommendation 6
Analgesics, such as paracetamol and opioid-(like) drugs, might be considered for residual pain after previously recommended treatments have failed, are contraindicated, and/or poorly tolerated.
This recommendation, driven by expert opinion, remained unchanged, due to the lack of trials on analgesics in axSpA. While short-term use of opioid-(like) drugs may have an acceptable risk–benefit profile, caution is advised for long-term use, which is in general not recommended.71 The ambivalence about this recommendation with the risk of addiction without proven efficacy in axSpA is also reflected in the lowest LoA among all recommendations (although still high). Given that residual pain is a frequent problem encountered in clinical practice, trials should be conducted to provide the necessary evidence, with the recommendation adapted as appropriate. Approach to pain management can also be guided by specific EULAR recommendations.72
Recommendation 7
Glucocorticoid injections directed to the local site of musculoskeletal inflammation may be considered. Patients with axial disease should not receive long-term treatment with systemic glucocorticoids.
This recommendation, also unchanged, addresses the use of glucocorticoid injections as an option to treat local inflammation (figure 1). Even though glucocorticoid injections have not been tested on arthritis or enthesitis in patients with axSpA, task force members are of the opinion that they can be efficacious. Local site injections, possibly guided by ultrasound, also refer to injections of the SIJ, which showed improvement in pain, though only tested in very small and old trials.73 74 Notwithstanding, a definite answer on the efficacy of SIJ injections based on low risk of bias trials is still needed.
Regarding systemic glucocorticoids for purely axial disease, evidence exists on short-term glucocorticoids only. Two studies suggest that short-term high-dose glucocorticoids (50 mg/day or 60 mg/day tapered over 24 weeks) could have a modest effect on signs and symptoms in patients with purely axial disease.14 75 76 Data on prolonged use of glucocorticoids in axSpA are lacking and, due to their known adverse events, the task force does not support their chronic use for axial disease.
Recommendation 8
Patients with purely axial disease should normally not be treated with csDMARDs; sulfasalazine may be considered in patients with peripheral arthritis.
The SLR retrieved no relevant new data on csDMARDs, and therefore this recommendation remained the same.14 csDMARDs are not recommended for purely axial disease due to their lack of efficacy, which has been shown for sulfasalazine, methotrexate and leflunomide.77–79 However, methodological shortcomings hamper the interpretation of trials with csDMARDs and, most importantly, there is a dearth of such trials and of relevant outcomes tested. Other treatment options for purely axial disease after failing NSAIDs are bDMARDs or tsDMARDs, which are costly and consequently not always available. Therefore, the task force agreed on emphasising that csDMARDs are normally not used, giving room for their exceptional use, as long as this is aligned with the OAPs, that is, ensuring the ‘best care’ and in shared decision with the patient. In patients with peripheral arthritis, however, csDMARDs are indicated with sulfasalazine being the preferred option due to its demonstrated efficacy in the subgroup of patients with peripheral arthritis, unlike methotrexate which has not demonstrated efficacy.77 78
Recommendation 9
TNFi, IL-17i or JAKi should be considered in patients with persistently high disease activity despite conventional treatments ( figure 2 ); current practice is to start a TNFi or IL-17i.

ASAS-EULAR recommendations for the treatment of patients with axial SpA with b/tsDMARDs. *Radiographic sacroiliitis is mandatory for drugs only approved in case of its presence; at the moment of the formulation of the recommendations: infliximab and JAKi. ASAS, Assessment of SpondyloArthritis international Society; ASDAS, Ankylosing Spondylitis Disease Activity Score; bDMARD, biological disease-modifying antirheumatic drug; CRP, C reactive protein; JAKi, Janus kinase inhibitors; MRI-SIJ, MRI of the sacroiliac joints; NSAIDs, non-steroidal anti-inflammatory drugs; SpA, spondyloarthritis; tsDMARD, targeted synthetic disease-modifying antirheumatic drug.
After failure of conventional therapy, treatment intensification should be considered for patients with persistently high disease activity. Figure 2 summarises the important eligibility criteria of patients to the next step in the treatment algorithm. It has previously been shown that adhering to the ASAS-EULAR recommendations for the initiation and continuation of TNFi leads to better functional outcomes and fewer days of sick leave.80
As indicated earlier, the task force considered it important to repeat that the first aspect is a clinical diagnosis of axSpA. The second aspect of the eligibility assessment deals with the presence of criteria that have been either associated with a higher likelihood of response or have been mandated by regulatory authorities. They are listed in decreasing order of the strength of predicting treatment response, namely elevated CRP, followed by presence of inflammation on MRI-SIJ, followed by the presence of radiographic sacroiliitis (according to the modified New York grading: grade ≥2 bilaterally or ≥3 unilaterally). Both elevated CRP and presence of MRI-SIJ inflammation should be related to axSpA, meaning that other plausible causes for such abnormalities should be carefully excluded. Elevated CRP has been identified as the strongest predictor of good response to TNFi therapy, both in patients with r-axSpA and nr-axSpA.81–84 In addition, inflammation on MRI-SIJ appeared to be the second best predictor of response to TNFi therapy, again irrespective of the presence of radiographic sacroiliitis.84–86 Lastly comes the presence of radiographic sacroiliitis, although not being predictive of response,7 87 but in order to comply with regulatory approval. When TNFi were historically approved for r-axSpA, no other conditions beyond active disease were mandated. It was only much later, when dealing with the approval of TNFi for nr-axSpA, that these drugs were restricted to patients with either elevated CRP or positive MRI-SIJ, given the higher response in patients with these objective signs of inflammation.84 However, with increasing knowledge of the predictive response of these factors in r-axSpA, the task force now recommends that CRP and (when available) MRI-SIJ are taken into account when deciding to start a b/tsDMARD, irrespective of the presence of radiographic sacroiliitis.83–86 Of note, at the time of the formulation of the recommendations, radiographic sacroiliitis was mandatory for infliximab and JAKi, which were only approved for r-axSpA. In the meanwhile, upadacitinib has been approved for nr-axSpA by the European Medicines Agency.88
Step 3 in the eligibility assessment refers to the failure of conventional treatment. This means non-pharmacological treatment and the use of at least two NSAIDs, in the maximum dose used in axSpA, over a total period of 4 weeks.89 In patients with predominantly peripheral manifestations, following recommendations 7 and 8, failure to treatment includes one glucocorticoid injection, if appropriate, and the use of sulfasalazine.
The following step focuses on the level of disease activity. Given the clear advantages of the ASDAS as described in relation to recommendation 2, the task force considers it to be the appropriate disease activity instrument, an observation that has been consolidated over the last decade. The task force therefore decided that high disease activity should be based on the ASDAS ≥2.1 criterion alone. If it is impossible to follow this recommendation, the BASDAI criterion (≥4) can be used as an alternative. There is a high agreement between both criteria but, in case of discordance, the ASDAS selects patients with a higher likelihood of response to treatment.90–92 In any case, the judgement of high disease activity should not be solely based on a score but complemented by the rheumatologist’s opinion, which should favour the start of a b/tsDMARD. Like any therapeutic decision, this should also follow OAP D and be part of shared decision-making with the patient.
In patients with persistently high disease activity despite conventional treatment, as defined above, TNFi, IL-17i or JAKi should be considered (figure 1). All these drug classes have demonstrated efficacy in axSpA trials.13 14 In the absence of head-to-head trials, it is difficult to prioritise any of them in terms of efficacy on axial disease. In the second part of the recommendation, the focus is placed on current practice, which is to start a TNFi or an IL-17i. This recommendation reflects the longer experience with the use of these drugs, with a larger evidence base, use in patients with multimorbidity (frequently excluded from randomised controlled trials (RCTs)) and more knowledge about drug safety.13 14 18 This decision is analogous to the previous recommendations, in which ‘current practice’ at that time was to start with a TNFi, for the exact same reasons, while IL-17i were already available. In addition, as only IL-17A inhibitors have so far been approved, reference to IL-17i is limited to IL-17Ai. Dual inhibition of IL-17A and IL-17F with bimekizumab has been tested in a phase II trial,93 but more information is needed about its efficacy and safety profile before it can be taken into consideration. For JAKi, at the moment, we only have RCT data, and only in r-axSpA. Data on nr-axSpA are currently underway, but not publicly available at the time of the formulation of the recommendations. Importantly, observational data and experience from daily clinical practice with JAKi in axSpA are missing, thus precluding the consideration of JAKi in ‘current practice’ part of the recommendation. In the future, observational data and experience with JAKi should help in addressing concerns with regard to safety, such as those identified with tofacitinib in patients with rheumatoid arthritis (RA). Tofacitinib has been associated with a higher risk of major adverse cardiovascular events (number needed to harm (NNH) for 5 mg two times per day tofacitinib of 113 over 5 years) as well as malignancies (NNH 55 over 5 years), when compared with TNFi. The trial was performed in patients with RA who were at least 50 years old and had at least one cardiovascular risk factor, and the risk was higher in patients over 65 years.94 During drug development, increases in serum lipid levels and the incidence of cancers, including lymphoma, were observed, prompting further investigation.95 96 In axSpA, such signals have not been described to date.14 97–99 Possible explanations for this include the younger age of patients with axSpA and their likely lower risk factor profile (including less comorbidities and less use of glucocorticoids), shorter follow-up and efficacy trials not enriched for a high-risk population.98 100 It is therefore unclear whether the increased risk of cardiovascular events and malignancies is specific to RA, and whether it will apply to axSpA, as well as whether they are specific to tofacitinib or reflect a JAKi class effect. Until more data become available, the task force recommends being restrictive with starting JAKi in patients above the age of 50 years with one or more additional cardiovascular risk factors and to those above the age of 65 years.
In this entire document, we refer to both original and biosimilar bDMARDs. Currently, biosimilars are available for TNFi. Taking OAPs into account, costs should be considered when choosing a particular drug. Given the similar expected efficacy and safety, cost is potentially an important consideration in choosing between an original and biosimilar bDMARD. This choice is increasingly determined by payers, and based on cost considerations, rather than by rheumatologists or patients. Cost may also drive the choice between an IL-17i and a (biosimilar) TNFi.
Aside from the importance on deciding when a patient is eligible for treatment with b/tsDMARDs, it is important to also decide on whether treatment is efficacious, and therefore appropriate to continue. Figure 3 summarises the criteria for continuation, namely that after at least 12 weeks of treatment, the disease activity has substantially decreased, as assessed by the ASDAS clinical important improvement, that is, improvement in ASDAS ≥1.1, together with the positive opinion from the rheumatologist to continue.40 As always, the final decision on whether to continue the treatment or not is made as a shared decision with the patient. As for the start of treatment, ASDAS is recommended for the assessment of response to treatment. If not possible to follow this recommendation, BASDAI response (≥2.0) can be used if BASDAI has been used to guide treatment initiation.

{kind=link}
{kind=link}
{kind=link}
ASAS-EULAR recommendations for the continuation of b/tsDMARDs. ASAS, Assessment of SpondyloArthritis international Society; ASDAS, Ankylosing Spondylitis Disease Activity Score; bDMARD, biological disease-modifying antirheumatic drug; tsDMARD, targeted synthetic disease-modifying antirheumatic drug.
Recommendation 10
If there is a history of recurrent uveitis or active IBD, preference should be given to a monoclonal antibody against TNF. In patients with significant psoriasis, an IL-17i may be preferred.
An important element of differentiation across the treatment options is their effect on EMMs13 leading to this new recommendation. In patients with previous uveitis, monoclonal antibodies against TNF (infliximab, adalimumab, certolizumab pegol, golimumab) have been shown to be efficacious in preventing the recurrence of uveitis, whereas etanercept showed contradictory results.101–107 In comparative analyses from registry data, monoclonal antibodies have been shown to be more efficacious in preventing an uveitis flare than etanercept or secukinumab.108 109 Additionally, secukinumab has been tried, unsuccessfully, in patients with non-infectious uveitis.110 These data led the task force to recommend monoclonal antibodies in patients with a history of recurrent uveitis (figure 1). Of note, this recommendation is meant to support treatment choice in those patients who have frequent and recent episodes of uveitis. In patients with IBD, existing data point in a similar direction, namely the efficacy of monoclonal antibodies against TNF and the lack of efficacy of etanercept and secukinumab.111–116 Thus, monoclonal antibodies are also preferred in patients with IBD. IL-17i are contraindicated in patients with active IBD. Although there are no specific comparative data on psoriasis in patients with axSpA, there are clear data on PsA. Two head-to-head trials have been conducted comparing IL-17i (secukinumab and ixekizumab) with TNFi (adalimumab in both trials), showing superiority of IL-17i in the achievement of robust skin outcomes.117 118 Therefore, an IL-17i may be preferred in patients with significant psoriasis.
Recommendation 11
Absence of response to treatment should prompt re-evaluation of the diagnosis and consideration of the presence of comorbidities.
Making an appropriate diagnosis of axSpA is not always straightforward. A good response to a bDMARD or JAKi in retrospect may suggest that the diagnosis of axSpA is correct. The task force here reiterates that the absence of clinical response should alert the physician to re-evaluate the patient: instead of a straight switch to a different immunosuppressive treatment, it seems wise to question whether the former diagnosis was indeed correct (figure 1). Striving for earlier diagnoses, as we nowadays do, may have advantages but also implies that more patients with relatively milder disease, less clear and classic symptoms and a better prognosis will be recognised, and misdiagnosis is increasing. In the past years, many efforts have been made in order to increase the awareness of the disease to try to reduce the diagnosis delay (that still exists), but nowadays rheumatologists should also be aware of the risk of misdiagnosis, overdiagnosis and overtreatment.119
Additionally, the presence of comorbidities, such as (but not restricted to) fibromyalgia, depression or osteoarthritis, is known to be associated with higher perceived disease activity, particularly if assessed exclusively by PRO measures, and also associated with poorer treatment outcomes.120–126 The task force therefore stipulated that the presence of comorbidities should be taken into consideration in the case of absence of response to treatment. A positive rheumatologist’s opinion to start treatment with a b/tsDMARD (figure 2) that complements an assessment of high disease activity, as described in recommendation 9, should therefore take possible comorbidities and their impact on disease activity assessment into account. This recommendation is also in line with a EULAR initiative on difficult-to-treat RA.127
Recommendation 12
Following a first b/tsDMARD failure, switching to another bDMARD (TNFi or IL-17i) or a JAKi should be considered.
The expansion of the treatment armamentarium for axSpA, now with three efficacious b/tsDMARD drug classes, each class with several options, opens more possibilities in the treatment of patients. When one treatment fails and the patient still fulfils the criteria to start a new treatment, a switch should be considered (figure 1). However, the evidence in terms of the efficacy of a given drug (class) after failure of a previous one is very limited. No RCT has been conducted with TNFi in patients failing a first TNFi, that is, TNFi-insufficient responders (TNFi-IR).13 Observational data suggest that a second TNFi can still be efficacious in TNFi-IR patients, although the level of efficacy may be lower than with the first TNFi.128 IL-17i have shown to be efficacious in TNFi-IR patients, also with a lower efficacy than in TNFi-naïve patients (direct comparisons only available for secukinumab).13 129–134 Data on JAKi separately in bDMARD-IR were not available at the time of the formulation of the recommendations. There are no data on the efficacy of TNFi after IL-17i or JAKi failure, neither on IL-17i in the case of JAKi failure nor JAKi in the case of TNFi or IL-17i failure. All these treatment sequences should be formally investigated and are therefore part of the research agenda (box 1). In the absence of data showing superiority of switching between different modes of action rather than within the same one, the task force agreed to recommend any switch, keeping all options open, but again taking the precautions for the use of JAKi as described for recommendation 9 (figure 1).
Research agenda
Treatment target in axSpA or for different disease presentations
Combined clinical and imaging target: superiority to clinical target only?
Assessment of disease activity in patients with fibromyalgia or other causes of chronic pain
Management of peripheral manifestations
Effect of physiotherapy on disease outcomes
Head-to-head comparisons between treatment options (TNFi, IL-17i and JAKi)
Efficacy of switches between different drug classes (switch in case of IL-17i failure or JAKi failure)
Impact of comorbidities on treatment response
Effect of the different drugs on EMMs
Effect of the different drugs on peripheral manifestations
Effect of treatment (NSAIDs, TNFi, IL-17i, JAKi) on structural damage progression
Effect of treatment (NSAIDs, TNFi, IL-17i, JAKi) on SIJ structural damage progression in patients with nr-axSpA
Impact of objective inflammatory markers (CRP+/MRI+) on b/tsDMARD response in r-axSpA
Efficacy and safety of b/tsDMARDs versus NSAIDs in patients without symptoms of the disease but with CRP+ and/or MRI+
Effect of therapeutic drug monitoring in treatment with bDMARDs, especially TNFi
Predictors of response to different drugs/drug classes
Efficacy of drugs stratified by gender
Role of exercise in patients with a high mechanical load (eg, due to job type)
Potential harmful effects of excessive exercise (on structural damage)
Management of residual pain
Further safety data of TNFi (observational studies)
Safety of IL-17i (observational studies)
Safety of JAKi (observational studies)
Safety of IL-17i and JAKi during pregnancy
Efficacy and safety of combinations of bDMARDs and tsDMARDs
Tapering of IL-17i and JAKi
Definition of sustained remission
Benefits and harms of T2T in axSpA
Role of imaging in monitoring of axSpA—additional value of MRI spine/SIJ, ultrasound/MRI of enthesis for treatment decisions
Impact of tapering b/tsDMARDs on structural damage progression
Efficacy of short-term glucocorticoids
Biomarkers of prognosis
Biomarkers of treatment response
Strategy trials
Start of tapering of b(ts)DMARDs, which criteria?
Efficacy and safety of analgesics for residual pain in axSpA
Difficult-to-treat axSpA: definition, best approach to management
axSpA, axial spondyloarthritis; bDMARD, biological disease-modifying antirheumatic drug; CRP, C reactive protein; EMMs, extramusculoskeletal manifestations; IL-17i, interleukin-17 inhibitors; JAKi, Janus kinase inhibitors; nr-axSpA, non-radiographic axSpA; NSAIDs, non-steroidal anti-inflammatory drugs; r-axSpA, radiographic axSpA; SIJ, sacroiliac joints; T2T, treat-to-target; TNFi, tumour necrosis factor inhibitors; tsDMARD, targeted synthetic disease-modifying antirheumatic drug.
Recommendation 13
If a patient is in sustained remission, tapering of a bDMARD can be considered.
An accumulating body of evidence shows that abrupt bDMARD withdrawal may lead to a high proportion of flares, while tapering was shown to be successful in maintaining treatment response.13 18 135–138 One double-blind trial with certolizumab in axSpA compared all three possible actions (continuing vs tapering vs stopping) directly and showed a significantly lower risk of flare for those who continued or tapered, compared with those who stopped.139 Tapering has been mostly studied through spacing drug administration.13 Although sustained remission has not been formally defined, in line with the advantages of the ASDAS previously mentioned, ASDAS inactive disease or low disease activity could be used here. ‘Sustained’ has not been defined either, but the task force considered it appropriate to emphasise that before starting to taper treatment, a patient should be in remission for a minimum period and that period should be (arbitrarily) at least 6 months. Existing data on tapering were restricted to TNFi.13 For IL-17i, there was only one study with withdrawal of ixekizumab leading to a high proportion of flares and no data on withdrawal or tapering of JAKi.13 14 140 The task force therefore decided to leave this recommendation unchanged and restricted to bDMARD tapering (figure 1). Importantly, tapering should be done steadily, with new assessments of the patient before moving further with a next step in the tapering approach. Tapering may ultimately result in discontinuation. During the whole process, OAPs should be followed, with ‘best care’ and ‘shared decision’ being key here.
Recommendation 14
Total hip arthroplasty should be considered in patients with refractory pain or disability and radiographic evidence of structural damage, independent of age; spinal corrective osteotomy in specialised centres may be considered in patients with severe disabling deformity.
This recommendation, unchanged from before, aims at raising awareness into potential surgical indications for problems associated with severe axSpA. Hip involvement is a frequent problem in patients with axSpA and symptomatic destruction should lead to the consideration of a total hip arthroplasty, regardless of the patient’s age.141 Especially in young patients, cementless prostheses are preferred.14 142 Patients with severe and disabling spinal deformity may be referred to a specialised surgeon so that corrective osteotomy can be considered.143 144
Recommendation 15
If a significant change in the course of the disease occurs, causes other than inflammation, such as a spinal fracture, should be considered and appropriate evaluation, including imaging, should be performed.
The final recommendation was kept unchanged and focuses on a (sudden) significant change in the course of the disease, which should trigger a comprehensive assessment of causes other than inflammation. In such a situation, a spinal fracture should be suspected, particularly in patients with ankylosis of the spine, as a fracture is then more likely to occur even with a minor trauma and usually leads to a worse outcome compared with a spinal fracture in the general population.145 When suspected, appropriate imaging such as MRI and/or CT scanning should be performed, and an experienced spinal surgeon may need to be consulted.146
Research agenda
The SLRs conducted to inform these recommendations highlighted existing gaps in the literature, which together with key discussion points raised during the task force meeting, resulted in our proposed research agenda (box 1).
Discussion
The ASAS-EULAR recommendations for the management of axSpA have been updated into a set of 5 OAPs and 15 recommendations covering both nr-axSpA and r-axSpA and including non-pharmacological and pharmacological treatment.
Since the last update in 2016, more data have become available on existing treatment options, and particularly on IL-17i. More data on secukinumab as well as on ixekizumab can now be considered, while the latter was not approved for axSpA at the time of the previous recommendations. For both, IL-17i efficacy has been shown not only in r-axSpA but also in nr-axSpA.13 In addition, JAKi represent a completely new drug class in these recommendations, with efficacy demonstrated for tofacitinib and upadacitinib in r-axSpA.14 The increasing availability of more drugs and with different modes of action raises questions around their positioning in the treatment pathway. With the lack of relevant head-to-head trials to date in axSpA, and with efficacy on axial disease seemingly similar across existing drugs, there are no reasons for prioritising one or the other in terms of efficacy. In this context, given the importance of EMMs in the treatment of axSpA and the distinctive effect of the different drugs on EMMs, a new recommendation has been formulated based on existing evidence: in patients with a history of recurrent uveitis or active IBD, monoclonal antibodies against TNF are preferred, while in patients with significant psoriasis, IL-17i are prioritised.13 14 The latter aligns with the EULAR recommendations for PsA, also giving preference to an IL-17i in case of significant skin involvement.147
In addition to efficacy, drug safety is a central aspect in treatment decisions. The more recently approved drugs naturally have less accumulated safety data. Observational studies include more ‘real-life’ patients, for example, with multimorbidity, who tend to be excluded from RCTs and are particularly informative for safety analyses, by allowing for more appropriate comparisons between interventions regarding long-term safety. Unlike in RA where there is a long history of robust observational data, for example, from registries,148 149 in axSpA (long-term) safety data are generally scarce and almost exclusively on TNFi. Safety data from IL-17i and JAKi are only available from RCTs.13 14 To date, the long-term safety of JAKi is challenged by the recently reported increased risks of major cardiovascular events and malignancies in patients with RA treated with tofacitinib compared with TNFi.94 Trials with a safety primary endpoint have not been conducted in axSpA and one cannot exclude that lack of statistical power is the reason that such safety signals have not been shown in current axSpA trials. It is therefore crucial to clarify whether these safety issues also apply to patients with axSpA and whether they represent a JAKi class concern. Until more solid data are available in axSpA, caution is advised. The task force wished to bring this aspect into the recommendations through the prioritisation of TNFi and IL-17i as first-line b/tsDMARD treatment in line with current practice.
The increasing number of effective, although expensive drugs with different modes of action stimulated much discussion by the task force. This is reflected in the OAPs, where the societal responsibility of rheumatologists is highlighted through the consideration of cost, while striving to provide the best level of care. Newer drugs coming into the market are more expensive than existing ones and this should be balanced against the expected added value, as perceived by patients.150
Recently, ASAS has issued quality standards to help improve the quality of healthcare provided to patients with axSpA.47 Expectedly, and also reassuringly, there are several points of connection between these OAPs and recommendations and the quality standards. For instance, non-pharmacological treatment, while addressed in one OAP and recommendation, is also reflected in two quality standards, emphasising its importance. Disease monitoring and frequent assessments, including a comprehensive annual review, are part of these recommendations and of the quality standards. These recommendations and ASAS quality standards can therefore be complementary and support clinical practice.
The clear selection of ASDAS as the instrument used to decide upon the eligibility of a patient for treatment with b/tsDMARDs (ASDAS ≥2.1), as well as about treatment continuation (improvement ≥1.1), represents an important novelty of these recommendations. With over a decade of extensive experience with ASDAS and the accumulated data evidencing its superiority, its choice was imperative.25 35 36 40 90–92 When it is not possible to use the ASDAS, it is better to use the BASDAI than no instrument at all, but we advocate that all efforts are made to implement the ASDAS in daily clinical practice.37 46
The task force extensively discussed the topic of treatment failure. Instead of the rather ‘simplistic’ approach of immediately starting a new DMARD once the former DMARD has failed, a careful and comprehensive assessment of the patient is recommended in order to avoid overtreatment.119 Among the possibilities for consideration are the correctness of the diagnosis and the presence of comorbidities that could influence disease assessment, treatment response or both. This is a new recommendation, driven by expert opinion and directly stemming from daily clinical experience. This, together with the high level of agreement within the task force, attests to the importance of this recommendation.
Peripheral manifestations of axSpA are increasingly recognised to be more frequent than initially thought.151–154 The assessment of treatment effects on peripheral manifestations has been suboptimal in axSpA, restricted to subanalyses of patients with peripheral involvement at study inclusion. So far, and in the absence of head-to-head comparisons, no differences have been identified in drug efficacy for peripheral manifestations. The task force considers the current recommendations to apply to patients with axSpA eventually presenting with peripheral manifestations. Notwithstanding, more research on tailored management of peripheral manifestations in axSpA is needed to inform future recommendations.
There are many similarities between the ASAS-EULAR and the American College of Rheumatology and SpondyloArthritis Research & Treatment Network recommendations.155 Indeed, it is the first time that the two sets of recommendations are thus aligned, which is reassuring in terms of the treatment of patients with axSpA worldwide. Differences are mainly in areas where strong evidence is lacking (eg, preferred choices when switching, tapering, T2T, spinal osteotomy). However, the format of the two sets of recommendations is substantially different: American recommendations are presented in elaborate detail (86 recommendations), with detailed treatment options and comparisons, while at the same time making the overview more challenging to follow as compared with the 5 OAPs and 15 recommendations from ASAS-EULAR. A few of the unique aspects of the ASAS-EULAR recommendations are: treating axSpA as a single disease, the explicit specifications in which a b/tsDMARD should be started and continued, the inclusion of JAKi as a drug class, treatment according to a target, treatment of axSpA in patients with significant psoriasis, non-pharmacological recommendation for treatment failure, tapering bDMARDs and cost considerations.
Implementation is a crucial aspect in the process of recommendations and that is often neglected.156 A dissemination strategy is currently underway which we hope will enhance the uptake and implementation of these recommendations. In the future, ASAS and EULAR could devote more efforts into implementation of recommendations, beyond their dissemination. Barriers and facilitators should be investigated as well as the uptake of the recommendations and quality standards should be measured to inform further strategies, both at a local and international level.
In conclusion, the 2022 update of the ASAS-EULAR recommendations provides healthcare professionals taking care of patients with axSpA, patients and other relevant stakeholders with the most up-to-date evidence and expert insights in the management of patients with axSpA. The next update is expected to be undertaken when sufficient new evidence has become available on existing or new treatment options. It is our vision that these recommendations standardise and optimise the treatment of people living with axSpA, contributing to both individual well-being as well as wider societal benefit through better management of the disease.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Handling editor Josef S Smolen
Twitter @ElenaNikiUK, @AlexSepriano, @PhilippeCarron, @pedrommcmachado, @annamolto, @michaelnissen, @ProftDr, @stezhao, @Nellziade
Contributors All authors were involved in the discussions and formulation of the recommendations. SR wrote the first version of the manuscript. All authors reviewed and commented extensively on the manuscript and approved the final version.
Funding EULAR and Assessment of SpondyloArthritis international Society (ASAS).
Competing interests SR received research grants from AbbVie, Galapagos, Novartis, Pfizer and UCB, and consulting fees from AbbVie, Eli Lilly, Novartis, MSD, Pfizer, UCB and Sanofi. EN has received speaker honoraria/participated in advisory boards for Celltrion, Pfizer, Sanofi, Gilead, Galapagos, AbbVie, and Lilly, and holds research grants from Pfizer and Lilly. AS has received speaker/consulting fees from UCB and Novartis. AO has nothing to declare. CW has nothing to declare. XB received consulting fees and research grants from AbbVie, BMS, Eli Lilly, Galapagos, Janssen, MSD, Novartis, Pfizer, Roche, Sandoz, Sanofi and UCB. XB is an editorial board member of Annals of Rheumatic Diseases. RBML received consulting fees from AbbVie, Bristol Myers Squibb, Celgene, Jansen, Galapagos, GlaxoSmithKline, Novartis, Pfizer, and UCB, and is director of Rheumatology Consultancy. FEVdB received consulting and/or speaker fees from AbbVie, Amgen, Eli Lilly, Galapagos, Janssen, MoonLake, Novartis, Pfizer and UCB. BB has nothing to declare. AB has nothing to declare. PC received consulting/speaker’s fees from Eli Lilly, Pfizer, AbbVie, Sanofi, Galapagos, Fresenius Kabi, Biogen, MSD, UCB and Novartis. AC received honoraria for lectures from AbbVie, Merck Sharp & Dohme and Novartis. FAvG received grants from Stichting ASAS, and consulting/speaker’s fees from Novartis, UCB, Pfizer, AbbVie, Eli Lilly, Bristol Myers Squibb and Celgene. PG received speaker’s fees from AbbVie. LG received consulting fees and research grants from AbbVie, Eli Lilly, Galapagos, Janssen, MoonLake, Novartis, Pfizer and UCB. JH has received speaker honoraria and participated in advisory boards for AbbVie, Lilly, Novartis and Janssen. MdH has nothing to declare. MH has received speaker’s fees from Novartis. UK has received grant and research support and consultancy fees from AbbVie, Amgen, Biocad, Biogen, Chugai, Eli Lilly, Fresenius, Gilead, Grünenthal, GSK, Janssen, MSD, Novartis, Pfizer, Roche and UCB. CL-M has received speaker/consulting fees from UCB, Novartis, Janssen, Eli Lilly, MSD and AbbVie. PMM has received honoraria from AbbVie, BMS, Celgene, Eli Lilly, Galapagos, Janssen, MSD, Novartis, Orphazyme, Pfizer, Roche, and UCB, and is supported by the National Institute for Health Research (NIHR) University College London Hospitals (UCLH) Biomedical Research Centre (BRC). HM-O received grants from Janssen, Novartis and UCB, and consultancy/speaker's fees from AbbVie, Biogen, Eli Lilly, Janssen, MoonLake, Novartis, Pfizer and UCB. AM received research grants from UCB and consulting fees from AbbVie, Biogen, BMS, Eli Lilly, Gilead, Novartis, MSD, Pfizer and UCB. VN-C received grants/honoraria from AbbVie, Galapagos, Janssen, Lilly, MoonLake, Novartis, Pfizer and UCB. MJN received grant from Novartis and consultancy/speaker's fees from AbbVie, Eli Lilly, Janssen, Novartis and Pfizer. FMP-S received research grants from AbbVie, Janssen, and Novartis, and consulting fees from AbbVie, Bial, Biogen, Eli Lilly, Janssen, MSD, Novartis, Pfizer, Pharma Kern, UCB and Tecnimed. DP received research support from AbbVie, Eli Lilly, MSD, Novartis, and Pfizer, and consulting fees from AbbVie, Biocad, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, MSD, MoonLake, Novartis, Pfizer, Samsung Bioepis, and UCB, and speaker's fees from AbbVie, Bristol Myers Squibb, Eli Lilly, Janssen, MSD, Medscape, Novartis, Peervoice, Pfizer and UCB. FP reports grants and personal fees from Novartis, Lilly and UCB, and personal fees from AbbVie, Amgen, BMS, Celgene, Janssen, Hexal, MSD, Pfizer and Roche. MR received consulting fees from AbbVie, Janssen, Eli Lilly, Novartis, Pfizer and UCB Pharma. MT has nothing to declare. SSZ has received consulting fees from UCB. NZ received research grants from AbbVie, Celgene, NewBridge and Pfizer; consulting fees from AbbVie, Eli Lilly, Pfizer, Gilead, Janssen, Novartis, NewBridge and Roche; and speaker's fees from AbbVie, Apotex, Eli Lilly, Janssen, Novartis, Pfizer, Pierre Fabre, Pharmaline, Roche and Sanofi-Aventis. DvdH received consulting fees from AbbVie, Bayer, BMS, Cyxone, Eisai, Galapagos, Gilead, GlaxoSmithKline, Janssen, Lilly, Novartis, Pfizer and UCB Pharma, and is director of Imaging Rheumatology.
Provenance and peer review Not commissioned; externally peer reviewed.