Article Text

Statistics from Altmetric.com
Chronic widespread pain (CWP) is associated with excess mortality. Robust evidence is provided in ARD by a study that included over half a million participants and a meta-analysis.1 This adds to the (already overwhelming) recognised burden of CWP and imposes an additional urgency in improving our understanding and management of the condition. Reducing excess mortality in patients with chronic pain requires an accurate knowledge of relevant mechanisms and mediators. Previous research and this new study indicate that this excess mortality is, to a large extent, explained by lifestyle factors such as decreased physical activity, increased body mass index, unhealthy diets and smoking. In this editorial, we will offer arguments and evidence emphasising the need to also take account of psychological factors to explain the link between CWP and early death.
Biopsychosocial model of chronic pain
Decades of research led to the current concept that chronic pain encompasses multiple and mutually interacting biological, psychological and social factors. These include—but are not limited to—nature of pain, peripheral and central pain processing mechanisms, physical disability, sleep disturbance, obesity, smoking, alcoholism and other health risks, psychological resilience and vulnerabilities (emotions, cognitions, behaviour) and social factors (work, support, facilities, financial resources). Relations between all factors of this biopsychosocial model are recognised to be dynamic and reciprocal, with mutually influencing pathways similar to a hanging mobile toy, in which movement of one component may induce change in all others and back. The weight of the distinct factors differs between individuals.
Psychological factors are important players in this context. To start with, they are core determinants of unhealthy lifestyles that turned out to be important in the recent study.1 For instance, reduced physical activity has been shown to be influenced by fear of movement-related pain (kinesiophobia)2 and by catastrophising cognitions (ie, rumination, magnification and helplessness).3 Lifestyle factors including unhealthy diet, excess weight and smoking are also (reciprocally) associated with psychological determinants. Thus, addressing the lifestyle factors contributing to increased mortality would certainly require consideration of the psychological dimensions affecting their adoption and correction. However, the potential roles of psychological dimensions in the link between CWP and mortality are more complex.
Psychological vulnerabilities predict excess mortality
Depression has been associated with increased all-cause mortality in a large variety of settings, from the general population (relative risk (RR) 1.524) to different disease conditions. Especially in cardiovascular disease, meta-analyses have demonstrated an association between depressive symptoms and the incidence of coronary events (RR 1.815), myocardial infarction (RR 1.326) and stroke (RR 1.457). Psychological stress and depression have also been associated with a higher incidence,8 faster progression9 and increased mortality10 of cancer.
In a hallmark study,11 it was shown that depression predicted risk of death in older persons. Early death was more likely in major than minor depression, but risk of death was still significantly higher in minor depression, even after correction for age, education level, chronic disease, smoking, obesity and sedentary lifestyle. In a study from the UK, over 68 000 members of the general population aged 35 years and over, at baseline free of cardiovascular disease and cancer, were included and followed up for an average of 8.2 years, accumulating more than 8000 deaths. A dose–response relation between intensity of psychological distress at baseline and mortality was shown, which remained significant after controlling for age, gender, comorbidity and behavioural and socioeconomic factors.12 Of note, this association was observed across the full range of distress, including people enduring common, subclinical levels of distress, who would not usually require mental health assistance.
Neuroticism has been directly and indirectly associated with a negative impact on a variety of health dimensions,13 including all-cause mortality.14 ,15 ,16 In the UK Health and Life-Style Survey publication of 2007,17 1 SD increase in neuroticism was associated with a 9% HR 1.09 (95% CI 1.03 to 1.16) increased risk of mortality from all causes.
Psychological resilience promotes longevity
Conversely, a variety of resilience factors has been identified that protect against early death. We will discuss optimism as an example of a cognition, positive affect and social support.
In a pivotal study, optimism was measured in a sample of 7007 college students.18 Forty years later, 91.1% of the most pessimistic students were still alive as compared with 94.1% of the most optimistic group. Similar results were observed in a recent publication of the Nurses Health Study19 involving more than 70 000 participants: a higher degree of optimism was associated with a lower mortality risk, which remained significant after adjustment for sociodemographic confounders, health behaviours, health conditions and depression (HR 0.91, 95% CI 0.85 to 0.97). The associations were verified for various causes of death, including cancer, heart disease, stroke, respiratory disease and infection. Data from a cohort of 602 Dutch elderlies, followed for 9 years, corroborated the view that optimism is associated with increased longevity.20
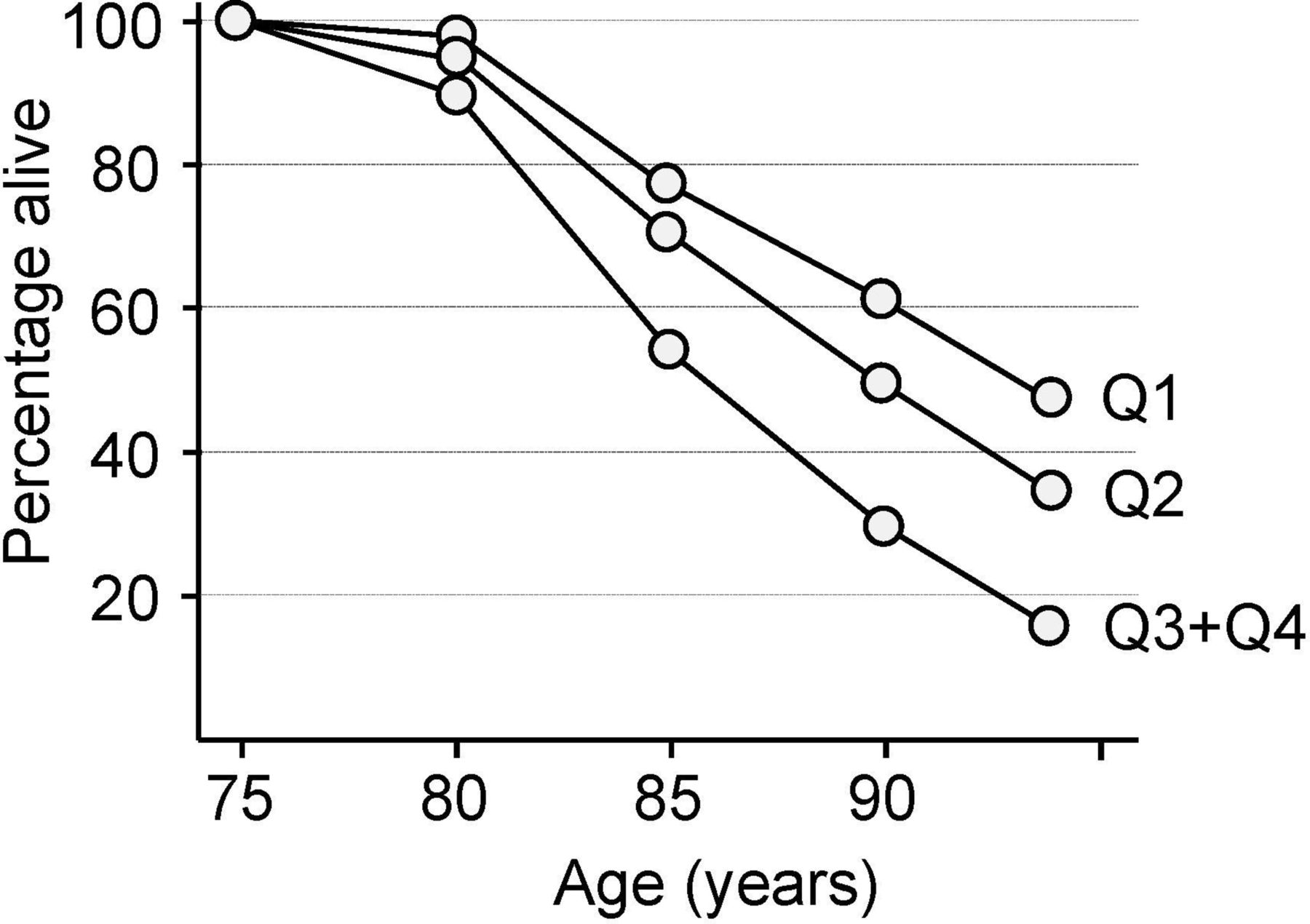
Also positive affect has been associated with increased longevity.21 ,22 A truly prospective study analysed handwritten biographies of 180 catholic nuns composed when the sisters joined the congregation at a mean age of 22.23 Emotion words in the biographies were counted and related to survival between ages 75 and 90. The results showed a strong positive correlation between the number and variety of positive emotional expressions in the early life biographies and longevity in later life, resulting in a 2.5-fold difference between the lowest and highest quartiles (figure 1). An important aspect of this study is that the nuns shared a very similar lifestyle, thus reducing its potential confounding role in the observations.

{kind=link}
Positive emotion expression at average age 22 and survival after age 75 years. Q1: highest quartile of number of positive emotion sentences; Q2: second highest quartile; Q3+Q4: quartiles 3 and 4 together (because of overlap), reflecting lowest number of sentences with positive emotions. Adapted from Danner et al.23
Findings of a pioneering study showed that social support predicted 30-month longevity in an elderly community population, even after controlling for age, sex, race, economic status, physical health status, self-care capacity, depressive symptoms, cognitive functioning, stressful life events and smoking.24 This finding has been consistently replicated in all kinds of groups. An interesting prospective study on mortality showed that providing social support may be even more beneficial than receiving it.25
Thus, overall, studies show that psychological vulnerability factors predict mortality but also that psychological resilience predicts longevity. All of these psychological factors are, to a certain extent, amenable to change, but how do they link CWP and mortality?
Psychological dimensions of CWP
Most accumulated evidence indicates that CWP is associated with a high prevalence of the vulnerability factors and a significant scarcity of the resilience factors described above. CWP has been consistently associated with an increased prevalence of a number of distressful psychological conditions, with emphasis on depression, anxiety and ‘overall’ negative affect.26 ,27 ,28 The annual prevalence of major depressive disorder among patients with fibromyalgia has been estimated at 22%, which is three times higher than in individuals without fibromyalgia.29 ,30 Other studies report even higher prevalence estimates.
Although CWP seems not strictly linked to a specific type of personality,31 some studies indicate that fibromyalgia is associated with higher rates of neuroticism.32 ,33 ,34 We have shown that healthcare professionals are able to distinguish patients with fibromyalgia from healthy controls, based solely on a limited set of items extracted from a personality profile, most being related to neuroticism.35
Depression, anxiety and neuroticism have well-established positive correlations with the prevalence and severity of pain, comorbid symptomatology and disability, in patients with CWP and in the general population.36 ,37 ,38 Psychosocial distress and stress have been identified as a predictor of new-onset CWP,39 ,40 and neuroticism has been shown to predict joint pain even over 23 years.41
Conversely, patients with CWP seem to present lower levels of resilience factors such as positive affect42 ,43 and social support.44 ,45 ,46 All of these risk and resilience factors have demonstrated correlations with daily intensity of fibromyalgia symptoms and have been the object of promising intervention studies in this context.
Clinical implications
The results presented by Macfarlane et al reinforce the evidence that CWP is associated with increased mortality of all causes, underlining the importance of developing our understanding of this condition to improve the care we provide to these patients. The complexity of the potential causative interactions underlying these observations cannot be overexpressed. Our editorial emphasises the importance of also attending to the psychosocial domains of CWP and their multifaceted potential consequences, including the mediation between CWP and increased mortality. This claim neither refutes the importance of lifestyle factors nor does it exclude the participation of yet additional risk factors, such as the adverse effects of non-steroidal anti-inflammatory drugs and other medications commonly used in this clinical context. The socioeconomic context also continues to deserve attention as it has been associated with both the prevalence of CWP47 ,48 and with higher overall cardiovascular and cancer mortality.49 Similar observations apply to sleep deprivation.50
We stress the potential importance of psychological domains, as they appear to have key influences in all ‘phases’ of these complex interactions, from the origin or maintenance of CWP, to the emotional and behavioural response to pain, the adoption of unhealthy lifestyles and the overall risk of death.
This is especially important in view of the efficacy of psychological therapies on CWP and its psychological correlates sleep problems, depression, functional status and catastrophising.51 A recent population-based intervention study52 demonstrated that a depression management programme significantly improved the long-term survival among older adults with high levels of medical comorbidity, which supports the view that targeting depression and other psychological correlates of CWP might decrease early mortality.
Conclusion
CWP should be seen as a biopsychosocial condition requiring a biopsychosocial understanding and therapeutic approach.
References
Footnotes
Contributors All authors contributed equally to the text through provision of ideas, writing, discussing and editing.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Clinical and epidemiological research