Article Text

Abstract
Background Peripheric Ulcerative Keratitis (PUK) is a severe inflammation that may lead to ocular perforation. PUK may be primary or associated with systemic conditions. Treatment is based on corticosteroids and conventional systemic immunosuppressive drugs.
Objectives To evaluate biologic therapy in cases with severe and refractory PUK.
Methods Multicenter study from 9 hospitals. Patients presented inadequate response or intolerance to conventional therapy with corticosteroids and at least 1 systemic traditional immunosuppressive drug.
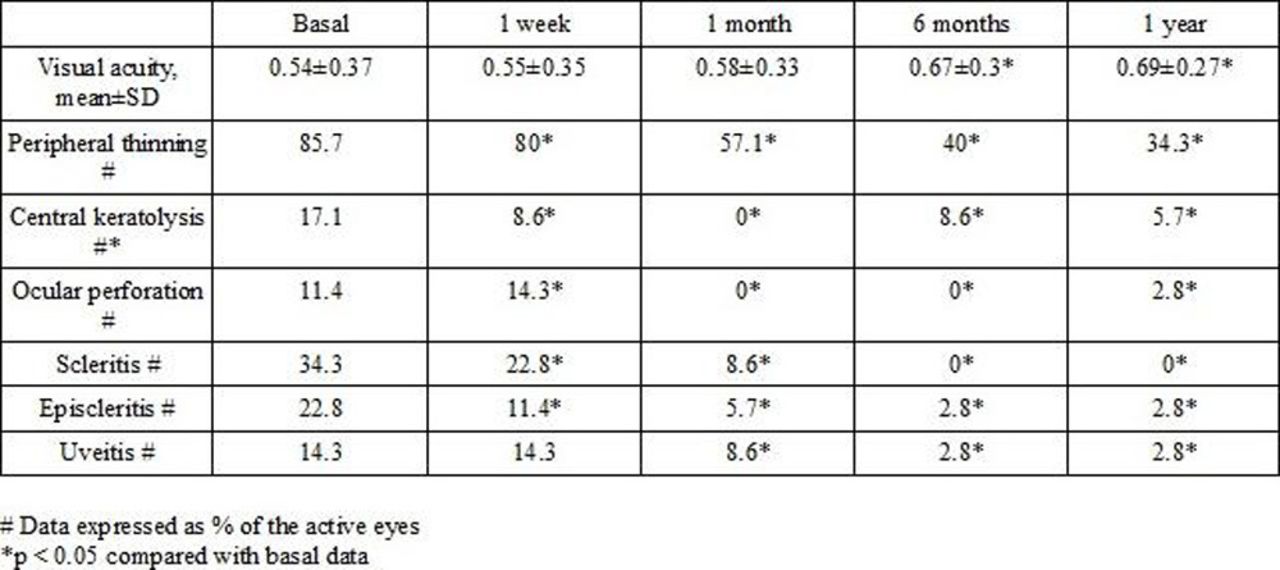
The main outcome measures were visual acuity, signs of inflammation, progression to corneal thinning, central keratolysis and ocular perforation. Comparisons were made between baseline and 1st week, 1st month, 6th month and 1st year. Statistical analysis was performed using the software STATISTICA (StatSoft). Results were expressed as mean±SD for variables with a normal distribution, or as median [IQR] when they were not normally distributed. The comparison of continuous variables was performed using the Wilcoxon test and categorical variables with chi-square test.
Results We studied 27 patients/35 affected eyes (7 men/20 women), mean age, 57.2±16.3 years (range 28–89). PUK was primary in 1 case whereas in the 26 remaining cases, the underlying diseases were Rheumatoid Arthritis (RA) (n=19), Psoriasic Arthritis (n=2), RA+Felty syndrome+common variable immunodeficiency (n=1), Behçet Disease (n=1), Type I diabetes mellitus (n=1), granulomatous polyangiitis (n=1) and microscopic polyangiitis (n=1). They received the following topical therapy: corticosteroids (n=18), antibiotics (n=17), lubricants (n=18), autologous serum (n=11), topical cyclosporin 2% (n=11) and topical tacrolimus 0.03% (n=1). Besides oral corticosteroids and before the onset of the biologic therapy they had received iv pulses of methylprednisolone (n=8), methotrexate (16), oral doxycycline (9), azathioprine (3) and ascorbic acid (2). Moreover, 10 patients required surgery: amniotic membrane (n=7), penetrating keratoplasty (n=4), conjunctival resection (n=3), tissue adhesives (n=2), conjunctival flap (n=1) and lamellar keratoplasty (n=1).
Anti-TNFα drugs were the most common biologic agents used in these cases (n=19): Adalimumab (ADA) (n=10; 37%), Infliximab (IFX) (n=8; 29.6%) and etanercept (n=1; 3.7%). In the remaining 8 cases the biologic agents were rituximab (n=7; 25.9%) and tocilizumab (n=1; 3.7%). The main outcome measures are summarized in the Table.
After a mean follow-up of 23.7±20 months, all objective outcomes had improved with a reduction of the median prednisone dose from 33.7 [17.5–52.5] mg at baseline to 0 [0–2.5] mg (p=0.028). The main observed adverse effects were supraventricular tachycardia (n=1) and pulmonary Tuberculosis (n=1).
{kind=link}
Conclusions In our series, biological therapy, especially IFX and ADA, is effective and relatively safe in patients with PUK refractory to standard systemic treatment.
Disclosure of Interest None declared