Article Text

Abstract
Objectives We used findings from the Global Burden of Disease Study 2013 to report the burden of musculoskeletal disorders in the Eastern Mediterranean Region (EMR).
Methods The burden of musculoskeletal disorders was calculated for the EMR's 22 countries between 1990 and 2013. A systematic analysis was performed on mortality and morbidity data to estimate prevalence, death, years of live lost, years lived with disability and disability-adjusted life years (DALYs).
Results For musculoskeletal disorders, the crude DALYs rate per 100 000 increased from 1297.1 (95% uncertainty interval (UI) 924.3–1703.4) in 1990 to 1606.0 (95% UI 1141.2–2130.4) in 2013. During 1990–2013, the total DALYs of musculoskeletal disorders increased by 105.2% in the EMR compared with a 58.0% increase in the rest of the world. The burden of musculoskeletal disorders as a proportion of total DALYs increased from 2.4% (95% UI 1.7–3.0) in 1990 to 4.7% (95% UI 3.6–5.8) in 2013. The range of point prevalence (per 1000) among the EMR countries was 28.2–136.0 for low back pain, 27.3–49.7 for neck pain, 9.7–37.3 for osteoarthritis (OA), 0.6–2.2 for rheumatoid arthritis and 0.1–0.8 for gout. Low back pain and neck pain had the highest burden in EMR countries.
Conclusions This study shows a high burden of musculoskeletal disorders, with a faster increase in EMR compared with the rest of the world. The reasons for this faster increase need to be explored. Our findings call for incorporating prevention and control programmes that should include improving health data, addressing risk factors, providing evidence-based care and community programmes to increase awareness.
- Epidemiology
- Low Back Pain
- Osteoarthritis
- Rheumatoid Arthritis
- Gout
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Musculoskeletal disorders have been underestimated and even ignored for a long time, mainly due to their low fatality rate and being viewed as irreversible conditions or simply part of the ageing process.1 The considerable contribution of musculoskeletal disorders is now more clear and several studies have quantified the significant burden of musculoskeletal disorders.2 They are among the most prevalent causes of absence from work and medical visits worldwide.2 High frequency, chronicity and resultant disability of musculoskeletal disorders impose a considerable economic burden on the communities. Population ageing is expected to dramatically increase the burden of musculoskeletal conditions over the coming decades.3 Despite these facts, musculoskeletal disorders have not been a focus of public health programmes, especially in low-income and middle-income countries.4
In the Eastern Mediterranean Region (EMR), epidemiological data on musculoskeletal disorders are sparse and not easily comparable. Most of the data in this region come from baseline surveys of the Community Oriented Program for Control of Rheumatic Diseases (COPCORD). The programme, designed by the WHO and the International League of Associations for Rheumatology in the 1980s, is presumably the most eminent public health programme to tackle the burden of musculoskeletal disorders in low/middle-income countries.5 Some countries in the EMR including Egypt, Iran, Kuwait, Lebanon, Pakistan and Tunisia have launched COPCORD projects in the past two decades.6 The COPCORD baseline surveys have shown a high prevalence of musculoskeletal conditions in the region; for instance, musculoskeletal complaints during the past seven days were reported by around 45% of people in Iran, based on four samples in rural and urban areas. The most common anatomical sites of symptoms were knees (27%), dorsolumbar spine (24%), shoulders (16%) and cervical spine (14%).7 Lifetime prevalence of musculoskeletal problems was reported by around 33% of people in Lebanon, with a current point prevalence of approximately 24%.8 About 27% of individuals in Kuwait reported musculoskeletal pain, and the most common sites of pain were knees, back and shoulders.9 In the northern part of Pakistan in 1997, 14.8% of people had rheumatic diseases with higher prevalence in rural areas (16.5%) compared with poor urban (13.6%) and affluent urban areas (10.7%).10 Musculoskeletal conditions (complaints or disorders) were generally more common in females compared with males.8–12 The overall prevalence of musculoskeletal conditions was higher in rural areas compared with urban.10 ,13 Original data from other countries of the region are usually limited to specific diseases.14–17 In the demographic and health survey of Palestine, 2% of the population reported a diagnosis of musculoskeletal diseases, with an increasing prevalence with age.18 Some of the countries in the region have no accessible original data on the magnitude and intensity of musculoskeletal disorders.
There is not a comprehensive summary or comparable data on the burden of musculoskeletal disorders in the countries of this region. In this report, which is part of the Global Burden of Diseases, Injuries, and Risk Factors Study 2013 (GBD 2013), we present the prevalence and burden of musculoskeletal disorders (low back pain, neck pain, osteoarthritis, rheumatoid arthritis, gout and other musculoskeletal disorders) at the regional and national levels in the EMR from 1990 to 2013, as well as the attributable burden from the known risk factors of musculoskeletal disorders.
Methods
GBD 2013 covers 188 countries, 7 super-regions and 21 regions from 1990 to 2013. In total, 306 causes of diseases and injuries, 240 causes of death and 79 risk factors were systematically analysed. Details on the methodology of GBD studies and the main changes to the methods for GBD 2013 have been explained in previous publications.2 ,19–21
There are 22 countries in the EMR by WHO designation with different levels of Gross National Income per capita. The low-income countries are Afghanistan, Djibouti, Somalia and Yemen; middle-income countries: Egypt, Iraq, Iran, Jordan, Lebanon, Libya, Morocco, Pakistan, Palestine, Sudan, Syria and Tunisia; and high-income countries: Bahrain, Saudi Arabia, Kuwait, Oman, Qatar and the United Arab Emirates.
In GBD 2013, the burden from six main categories of musculoskeletal disorders was calculated: rheumatoid arthritis, osteoarthritis, low back pain, neck pain, gout and other musculoskeletal disorders. We used the International Statistical Classification of Diseases and Related Health Problems, tenth revision (ICD-10) codes or their equivalent codes in the earlier versions of ICD and assumed different sequelae for each disorder (table 1). Each musculoskeletal disorder had a list of sequelae with potentially different levels of disability; for instance, low back pain had eight sequelae classified as mild, moderate, severe and most severe low back pain with or without leg pain. Range of disability weight for these sequelae was different from 0.02 (95% uncertainty interval (UI) 0.011–0.035) for mild low back pain without leg pain to 0.384 (95% UI 0.256–0.518) for most severe low back pain with leg pain. A complete list of health state descriptions and equivalent disability weights is available in the web appendix of a previous GBD publication.21
Musculoskeletal disorders, equivalent ICD-10 codes and list of sequelae for each disorder in the Global Burden of Disease Study
In this study, the burden is described as prevalence, deaths, years of life lost (YLLs) due to premature mortality, years lived with disability (YLDs) and disability-adjusted life-years (DALYs). We calculated crude and age-standardised rates to be able to distinguish the difference in population structure from the difference in age-specific and sex-specific rates.
Most of the musculoskeletal disorder categories (except rheumatoid arthritis and the category of ‘other musculoskeletal disorders’) were assumed to be non-fatal with no mortality and no YLLs due to premature mortality. To estimate the cause-specific deaths, all-cause mortality envelopes (total number of deaths due to any cause) were estimated for each country during the period of 1990–2013. All accessible data from vital registration systems, sibling history surveys, sample registration data and household recall of deaths were considered for preparing these envelopes. Cause of death data was extracted from the same sources, as well as any available verbal autopsies.19 We used cause of death ensemble modelling 22 to estimate the number of deaths from rheumatoid arthritis and ‘other musculoskeletal disorders’ by age, sex, country and year.
To estimate morbidity, we updated the GBD 2010 systematic reviews of epidemiological measures for each musculoskeletal disorder. We used different strategies to avoid missing sources of data, which included sharing of the results of systematic reviews with the extensive network of GBD collaborators.21 A list of GBD 2013 data citations is available on the Global Health Data Exchange tool (http://ghdx.healthdata.org/gbd-2013-data-citations). A series of Bayesian meta-regression analyses through DisMod-MR 2.0 were used for disease modelling. We used fixed effects for study-level and country-level covariates to adjust input data. As an example of study-level covariates, we included studies with standard OA disease definition as the reference standard and adjusted extracted data from other studies that define OA based on ‘reporting having had a diagnosis of OA’, ’radiographic diagnosis of OA regardless of symptoms’ or ‘OA with symptoms but no radiographic confirmation’. More details on covariates are available in the online appendix of a previous publication.21 Model-based epidemiological estimates in combination with disability weights were used to calculate cause-specific YLDs for each age, sex, location and calendar year.21 DALYs were calculated through summation of YLLs and YLDs.
We calculated attributable burden of the following risk factors from the total burden of musculoskeletal disorders: occupational ergonomic factors, high body mass index and low glomerular filtration rate. Details on definitions of these risk factors and their relative risk for musculoskeletal disorders are available in the web appendix of a previous publication.20
We have reported 95% UIs for each quantity in this analysis. The UIs are based on taking 1000 samples of posterior distribution and report the 25th and 975th values of the distribution.21
Results
The number of deaths due to musculoskeletal disorders in EMR increased from 1706 (95% UI 1380–2090) in 1990 to 5084 (95% UI 3794–5869) in 2013, a 198% increase. Age-standardised death rate was 0.89 per 100 000 (95% UI 0.74–1.15) in 1990 and 1.39 per 100 000 (95% UI 1.07–1.58) in 2013. The number of deaths in 2013 was equal to 0.83 crude deaths per 100 000 (95% UI 0.62–0.95) and constitutes 0.14% (95% UI 0.10–0.16) of all deaths. YLLs of musculoskeletal disorders increased from 68 211 (95% UI 52 961–86 586) in 1990 to 183 659 (95% UI 131 166–219 907) in 2013, a 169% increase.
Web appendix table S1 shows point prevalence of musculoskeletal disorders in the EMR countries. Low back pain was the most common condition in all countries in 2013, except Kuwait and Lebanon where neck pain was more prevalent: the range of point prevalence of low back pain was between 32.45 per 1000 in Kuwait and 159.23 in Egypt. The range of point prevalence of neck pain was between 34.31 per 1000 in Pakistan and >55 per 1000 in Somalia and Djibouti. Osteoarthritis ranged from 29.67 per 1000 in Pakistan to >46 per 1000 in Somalia and Djibouti. Point prevalence of gout had a range of 0.15 per 1000 in Pakistan to 1.00 per 1000 in Iran and Qatar. Point prevalence of rheumatoid arthritis was between 0.88 per 1000 in Saudi Arabia and >3 per 1000 in Somalia and Djibouti (web appendix table 1). YLDs of musculoskeletal disorders increased from 1279 per 100 000 (95% UI 907–1686) in 1990 to 1576 (95% UI 1111–2100) in 2013. Musculoskeletal disorders were the second leading cause of YLDs after ‘mental and substance use disorders’ and accounted for 15.7% of all YLDs (95% UI 13.8–17.7%) in 2013. Low back pain and neck pain had the highest YLDs among the disorders (web appendix 1).
supplementary web appendix table
As expected, YLDs were the main component of DALYs for musculoskeletal disorders (>98%, both in 1990 and 2013), and DALY estimates were very close to YLD estimates. The total burden of musculoskeletal disorders was 4 842 603 DALYs (95% UI 3 450 654–6 359 159) in 1990 and increased to 9 946 874 DALYs (95% UI 7 068 174–13 194 791) in 2013, a 105.4% increase in total DALYs of musculoskeletal disorders, compared with a 58.0% increase in the rest of the world. The crude DALYs rate per 100 000 increased from 1297.1 (95% UI 924.3–1703.4) in 1990 to 1606.0 (95% UI 1141.2–2130.4) in 2013, which shows a 23.8% increase. Age-standardised DALY rates were 2055.6 (95% UI 1478.3–2704.1) in 1990 and increased by 2.9% to 2115.9 (95% UI 1517.2–2799.7) in 2013. The burden of musculoskeletal disorders as a proportion of total DALYs has constantly increased since 1990; the proportion that was 2.4% (95% UI 1.7–3.0) in 1990 increased to 3.2% (95% UI 2.8–4.6) in 2000 and 4.7% (95% UI 3.6–5.8) in 2013. Figure 1 compares the burden of musculoskeletal disorders in the EMR to data for the world, low/middle-income countries and high-income countries. Table 2 summarises DALY rates for each musculoskeletal disorder. As shown, DALY rates have been increased during 1990–2013 for all musculoskeletal disorders, both in men and women.
Crude rates of disability-adjusted life-years (per 100 000) for musculoskeletal disorders in the Eastern Mediterranean Region, 1990 and 2013

Burden of musculoskeletal disorders in the Eastern Mediterranean Region compared with the world, high-income countries and developing countries, 2013. DALYs, disability-adjusted life-years.
Egypt had the highest and Lebanon had the lowest age-standardised musculoskeletal disorders DALY rates both for males and females. Ranges of age-standardised DALY rates had a considerable overlap between the low-income, middle-income and high-income countries of EMR (table 3).
Age-standardised disability-adjusted life year rates (per 100 000) of musculoskeletal disorders by country and sex in the Eastern Mediterranean Region, 2013
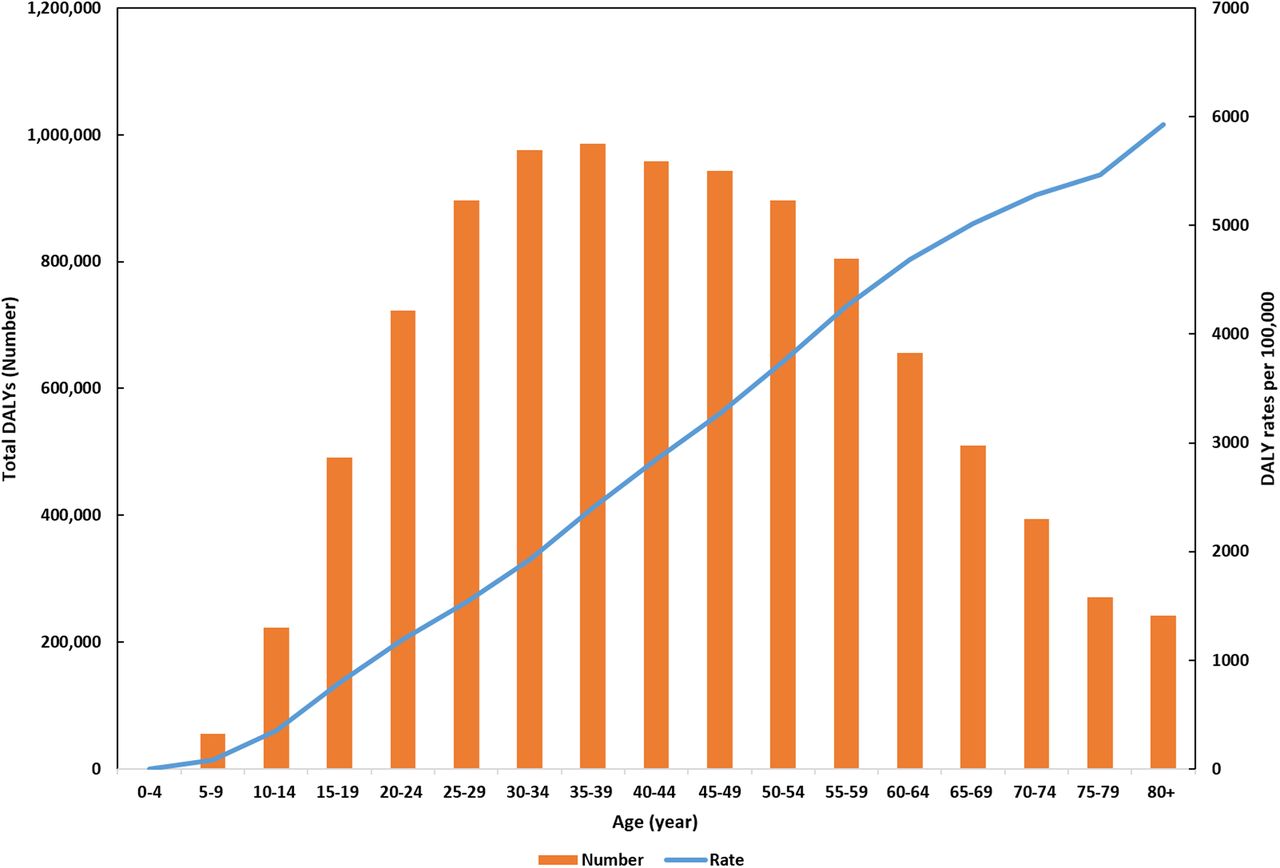
DALY rates had a clear increasing pattern with age; however, those of middle age had the highest number of DALYs (figure 2). Among different musculoskeletal disorders, low back pain had the highest proportion of DALYs in all age groups. The proportion of osteoarthritis DALYs out of total DALYs of musculoskeletal disorders increased with age. In individuals aged ≥65 years, osteoarthritis was the second important cause of DALYs after low back pain.

Age-specific rates and numbers of disability-adjusted life-years (DALYs) of musculoskeletal disorders in the Eastern Mediterranean Region, 2013.
The burden of musculoskeletal disorders was higher in females compared with males, except for low back pain and gout. The total burden was 5 415 756 DALYs (95% UI 3 877 474–7 150 503) in females and 4 531 118 DALYs (95% UI 3 200 432–6 026 689) in males in 2013. DALY rates were 1800.9 (95% UI 1289.4–2377.7) and 1422.2 (95% UI 1004.5–1891.6) in females and males, respectively. Figure 3 shows the burden of each musculoskeletal disorder by sex in 2013. Gout had a small burden (0.6 and 1.7 DALYs per 100 000 in women and men, respectively) and its burden has not been shown in the figure.

{kind=link}
{kind=link}
{kind=link}
The burden of musculoskeletal disorders in the Eastern Mediterranean Region by sex, 2013. DALYs, disability-adjusted life-years.
The ratio of age-standardised female to male musculoskeletal DALY rates ranged between 1.02 in Morocco and 2.01 in Iran (table 3). The ratio of age-standardised female to male DALY rates was <1 for gout disease in all countries of the region. For low back pain, the ratio was <1 except for Sudan (1.02), Egypt (1.03), Saudi Arabia (1.15), Lebanon (1.43) and Iran (1.76). Except the above-mentioned cases, for each country disorder, the ratio of age-standardised female to male DALY rates was >1.
Occupational ergonomic factors and high body mass index were the most important risk factors for musculoskeletal disorders. Around 1 545 221 (95% UI 1 023 600–2 148 137) DALYs of low back or neck pain were attributable to occupational ergonomic factors and 436 766 DALYs (95% UI 283 614–626 896) of its burden were attributable to high body mass index. Moreover, 462 676 DALYs (95% UI 313 110–642 108) of osteoarthritis burden were attributable to high body mass index. Occupational ergonomic factors were the most important risk factor in men, while high body mass index was a more important factor in women: the attributable burden to occupational ergonomic factors was 3.2 times of the attributable burden to high body mass index in men and 0.8 for women. This ratio had a range of 4.3–12.3 in the low-income countries of the region, 0.7–6.4 in the middle-income countries and 0.8–1.5 in the high-income countries of the region.
Discussion
This study shows high prevalence and burden of musculoskeletal disorders, especially for low back pain, neck pain and osteoarthritis in the region. The burden of these disorders has increased in the EMR more than the rest of the world during 1990–2013. Although the increase in burden is mainly related to increase in population size and ageing, despite most of the other diseases, there was no decrease in the age-standardised rates of burden. The proportion of musculoskeletal disorders' burden over total burden of disease has even increased. Musculoskeletal disorders are the second leading cause of disability in the EMR. Although population ageing is a main reason for increasing burden of musculoskeletal disorders, a large proportion of the burden is imposed on people in their most active and productive years of life. We did not find a specific association between income level of the country and burden of musculoskeletal disorders; however, the relative importance of risk factors (occupational ergonomic factors compared with high body mass index) was different based on the income level of countries.
Our findings call for incorporating prevention and control programmes for musculoskeletal disorders in national health programmes. COPCORD could be used as a stepwise approach to address the high burden of musculoskeletal disorders; however, previous COPCORD programmes in EMR usually have not progressed beyond the early stages (such as baseline surveys) towards a focus on prevention and control activities.6 ,23 Considering the important risk factors of musculoskeletal disorders, public education, occupational health and safety and ergonomics are among the most important components of any prevention and control programme. Medical interventions and rehabilitation to preserve functional status are essential to provide control of the situation.
Advocacy is required to raise the attention of policy and decision makers to the disease burden caused by musculoskeletal disorders.3 As a reflection on the previous round of the ongoing GBD study, some experts recommended extensive involvement of the local community to initiate any intervention for control of musculoskeletal disorders and integrating services with existing policies and structures.3 Mody and Brooks suggested new models of care and strategies to train community health workers and primary healthcare providers to detect and initiate the management of patients at earlier stages.24
The education of patients and the entire population, treatment with cost-effective interventions, prevention through identification and reduction of environmental and genetic risks are the main components of interventions after primary epidemiological assessments.23 ,25 People with musculoskeletal conditions are exposed to a spectrum of services including traditional, complementary and alternative therapies of which efficacies may not always be clear.26 Recent biological medications and surgical approaches are changing the long-term outcomes of some musculoskeletal disorders such as rheumatoid arthritis or severe osteoarthritis; however, they can be too expensive to be affordable in all countries.27 Timely access to healthcare providers is important for some of the musculoskeletal disorders. For instance, in patients with inflammatory disorders such as rheumatoid arthritis, early assessment by a specialist improves the prognosis.28 However, previous studies show that many individuals with musculoskeletal disorders do not receive treatment in EMR countries; in Lebanon, around a quarter of these individuals seek some kind of treatment.26 On the other hand, there is a high risk of using unnecessary diagnostic or therapeutic procedures for people with musculoskeletal symptoms, especially in the wealthier countries. This needs to be avoided through proper planning for quaternary prevention.
Modification of lifestyle factors (such as maintaining physical fitness and ideal weight, having a balanced diet, avoidance of smoking and excess alcohol consumption, and preventing injuries) is not only beneficial for musculoskeletal health but also for other non-communicable diseases that contribute to increasing mortality and morbidity.24
Low back pain and neck pain have the highest burden of musculoskeletal disorders in most of the EMR countries. In previous studies, the seven-day period prevalence of pain for dorsolumbar and cervical spine in Iran were 23.7% and 14.2%, respectively.7 The estimates were higher in rural areas compared with urban areas, and also in people with specific jobs and pregnant women.29 In Kuwait, the point prevalence of low back pain in schoolchildren aged 10–18 years old was 20.6% in males and 39.3% in females.30 A cumulative prevalence of around 28% for low back pain was reported by children aged 11–19 years old in Tunisia.31 Some of these estimates cannot be directly compared with our estimates due to different definitions and the time interval used for assessment. However, the available evidence collectively reflects the importance of the problem. There are several evidence-based public health and clinical guidelines for low back pain32–34 and neck pain,35 ,36 usually from high-income countries. Development of suitable guidelines for use in resource-poor settings is challenging. Most research evidence originates from high-income countries and may not be relevant or applicable to the needs of low-income countries. Moreover, the development of valid clinical guidelines needs resources and certain expertise that sometimes is not available. In the paucity of nationally developed guidelines, EMR countries can use the available guidelines through adaptation processes.37
Osteoarthritis is an important cause of disability, especially in elderly people. It is expected to be influenced by the population ageing process more than other musculoskeletal disorders. Some evidence suggests that intensive physical activity might increase risk of osteoarthritis in large joints; however, this is not a general conclusion.38 Findings on association of physical activity and osteoarthritis are especially confusing in the elderly; while some studies suggest that walking and physical exercise has a deleterious effect on osteoarthritis, there are some reviews that show aerobic exercises in elder individuals can help to reduce symptoms of knee osteoarthritis.39 Light or moderate physical activities are not usually known to increase risk or complications of osteoarthritis. Physical activity can also decrease risk of osteoarthritis through reducing body mass index.38 ,39 The burden of ‘other musculoskeletal disorders’ was around threefold in women compared with men. Conditions such as fibromyalgia and connective tissue disorders are more prevalent among women.7 ,8
Our study has some limitations. Although we estimated a collective burden for musculoskeletal disorders in this study, we did not provide separate estimations for some of the disorders such as spondylopathies and systemic connective tissue disorders. Moreover, we did not separately assess the burden of hand osteoarthritis. Our classification of musculoskeletal disorders does not have a distinction between symptoms, complaints and diseases; however, ICD-10 codes clarify the components of each category. We did not include osteoporosis as a disease; instead, low bone mineral density was classified as a risk factor for fractures, so its attributable burden has not been shown in this paper. Finally, we did not provide separate estimates for diseases such as the Behçet disease, which have regional importance in EMR or individual (but not collective) high burden.
There were issues with availability and quality of data in some EMR countries; however, we used GBD modelling approaches to reduce this issue. Indeed, the lack of high-quality data in the region, especially from the 1990s, might have an influence on the estimated trend of musculoskeletal diseases. Although this issue exists for many of the causes of diseases, it might have an imbalanced effect on musculoskeletal diseases (the importance of which has been highlighted in the recent decades) compared with the other diseases. This factor might affect different regions of the world in different ways. However, we do not believe that it can purely explain the faster increase in burden of musculoskeletal disorders in EMR compared with the rest of the world.
Conclusion
Findings from this study show a high burden of musculoskeletal disorders, especially low back pain, neck pain and osteoarthritis in the region. The reasons for faster increase of musculoskeletal disorders' burden in EMR during 1990–2013 compared with the rest of the world need to be explored. Our findings call for integrating prevention and control programmes for musculoskeletal disorders with health system programmes. Plans should include improving health data to monitor trends, addressing known risk factors especially through health education and awareness, ergonomics and occupational health and safety, and providing evidence-based early diagnosis and treatment, rehabilitative care and community programmes to increase knowledge of risk and protective factors.
Acknowledgments
The authors acknowledge Pauline Kim at the Institute for Health Metrics and Evaluation, Seattle, WA, for editing this paper.
References
Footnotes
Handling editor Tore K Kvien
Contributors MM-L and AHM prepared the first draft. All other authors provided data, developed models, analysed data, reviewed results, provided guidance on methodology and/or reviewed the manuscript. MM-L and AHM finalised the draft based on comments from other authors’ feedback. MM-L, AHM, AA and MHF responded the comments of reviewers. AHM and CJLM accept full responsibility for the work, have access to the data and controlled the decision to publish.
Funding The global burden of disease study was funded by the Bill and Melinda Gates Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.