Article Text

Abstract
Background Extracranial large vessel vasculitis (LVV) diagnosis is delayed compared to classical temporal arteritis. There is a need for simple and reliable tests for the diagnosis of extracranial large vessel giant cell arteritis (GCA). Identifying extracranial giant cell arteritis increases diagnostic specificity and adds prognostic value, as extensive vascular involvement may be associated with a poorer treatment response. Color duplex sonography (CDS) is most promising tool for the assessment of not only temporal but also large vessel arteritis. However, the proper interpretation of the vasculitis findings remain an important concern, as for an inexperienced ultrasonographer it remains elusive. There is still a need to define ultrasound findings, unify the diagnostic cut-offs and implement such standards by educating ultrasonographists.1,2
Objectives We present a novel idea to define a simple, sonographic sign of axillary arteritis.
Methods 214 consecutive patients suspected for GCA were included in the study between 2011 and 2015 and followed up for at least 0,5 year. Axillary arteries were scanned from axillary approach by continuing distally in a longitudinal plane down to brachial arteries. All examinations, together with categorization into arteritis and non-arteritis findings, were performed by a single physician with at least 5 years long experience in LVV ultrasound, that was blinded to diagnosis but aware of clinical presentation. Esaote MyLab25Gold Machine with 10 and 18 MHz linear probes was used.
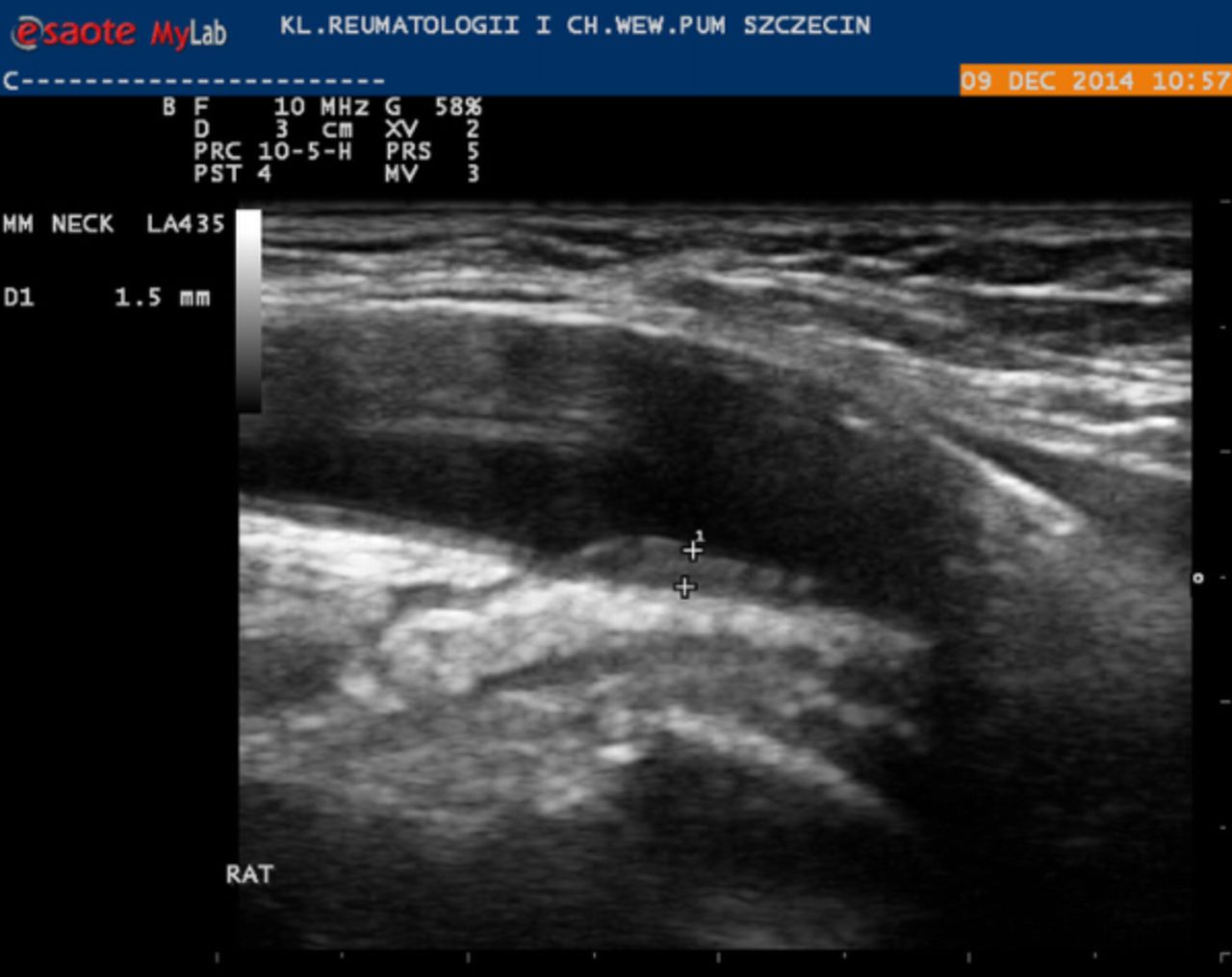
Slide sign was considered positive (Figure 1) if there was an increased axillary artery wall thickening, (hypoechoic, homogenous, with distorted wall structure resulting in no clear intima-media structure, usually circumferential, over long distance but not limited only to the place of arterial bifurcation), that was followed by a brachial artery without wall thickening and with normal IM structure (clear double line).
The diagnosis was based on ACR criteria (for cranial GCA), or presence of typical manifestations together with large vessel arteritis confirmed by whole aorta CT or ultrasound (for extracranial GCA). Non-GCA patients served as controls.
Results GCA was diagnosed in 81 patients. Extracranial LVV was diagnosed in 28 patients. Axillary vasculitis was diagnosed in 23 patients and was not found in controls. Positive slide sign was found in 23 patients. They've matched the patients with ultrasnographic signs of axillary vasculitis, so congruency between both methods was 100%.

{kind=link}
Conclusions Slide sign compared with large vessel halo sign serves at least non inferior diagnostic performance. Although qualitatively accessed slide sign does not bring additional diagnostic value over signs of axillary vasculitis it is easier to define and to observe.
This proposed definition of slide sign contains description of pathological findings in axillary artery, normal findings in brachial artery - which is typically not involved in vasculitis or involved only per continuum in a proximal part, and some features to help to exclude arteriosclerosis.
Czihal M et al. Impact of cranial and axillary/subclavian artery involvement by color duplex sonography on response to treatment in giant cell arteritis. J Vasc Surg. 2015;61:1285–91
Aschwanden M et al. Temporal artery compression sign–a novel ultrasound finding for the diagnosis of giant cell arteritis. Ultraschall Med. 2013;34:47–50
Disclosure of Interest None declared