Article Text

Abstract
Background MTX plus anti-TNF therapy is an effective treatment for early RA. It is becoming increasingly important to understand whether the dose of anti-TNF can be reduced or stopped in patients (pts) receiving long-term therapy.
Objectives To demonstrate that for patients (pts) who achieved sustained low disease activity (sLDA) after 1 year (yr) with CZP 200mg Q2W+optimized MTX, continuation of certolizumab pegol (CZP) as a standard (200mg Q2W) or reduced-frequency dose (200mg Q4W) is superior to stopping CZP for maintaining pts in LDA from Week (Wk) 52 through Wk104.
Methods CZP+MTX-treated pts achieving sLDA (DAS28[ESR]≤3.2 at Wks40 and 52) in C-EARLY Period 1 (NCT01519791)1 entered Period 2 (NCT01521923); pts were randomized 2:3:2 to CZP standard dose (200mg Q2W+MTX), CZP reduced-frequency dose (200mg Q4W+MTX) or CZP stopped (PBO+MTX). Pts were evaluated every 8–12 wks. The Period 2 primary endpoint was the proportion of pts who maintained LDA (DAS28[ESR]≤3.2) from Wk52 through Wk104 without flare, using non-responder imputation for missing values. CZP standard dose was compared with CZP stopped; if p<0.05 was achieved then, as per the hierarchical testing scheme, CZP reduced-frequency dose was compared with CZP stopped.
The assumptions were that 455 pts would achieve sLDA in C-EARLY Period 1 and enter Period 2, with a response of 95%, 90% and 75% at Wk104 for standard, reduced-frequency and stopped dose respectively. Given α=0.05, there would be 99% and 92% power to detect a difference between CZP standard and reduced-frequency dose vs stopped dose.
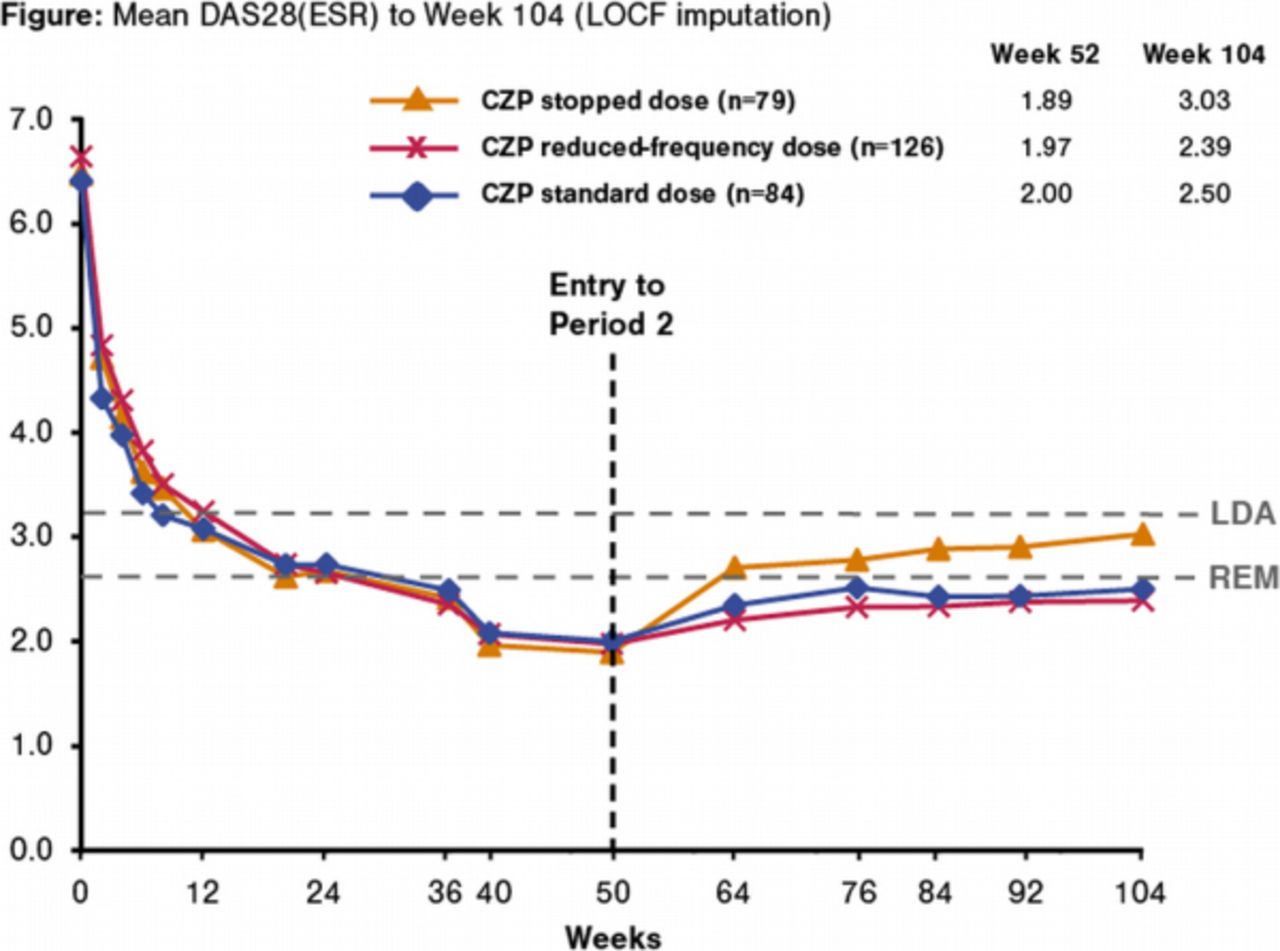
Results In Period 2, 289 pts (who had achieved sLDA in Period 1) were included in the full analysis set: CZP Q2W+MTX (n=84), CZP Q4W+MTX (n=126) or PBO+MTX (n=79). From Wk52 through Wk104, a greater proportion of pts continuing CZP (either Q2W or Q4W)+optimized MTX maintained LDA vs PBO+MTX (48.8% and 53.2% vs 39.2%; p=0.112 and p<0.05 [nominal p value; first hierarchical test not significant]). Pts stopping CZP tended to worsen over time, as demonstrated by the increase of the mean DAS28(ESR) values from 1.89 at Wk52 to 3.03 to Wk104 (Figure). No new safety signals were observed.
{kind=link}
Conclusions Early RA pts with prognostic factors for severe disease progression achieving sLDA after 1yr of standard dose CZP+optimized MTX can taper to CZP reduced-frequency dose and maintain comparable disease activity control to CZP standard dose. Pts who stopped CZP had a tendency to have more relapses; despite this, 39.2% of these pts maintained LDA through Wk104. Further work will aim to identify the characteristics of pts who can successfully stop CZP.
Weinblatt M. Arthritis Rheumatol 2015;67(S10)
Acknowledgement The authors acknowledge Costello Medical Consulting, funded by UCB Pharma, for writing and editorial assistance.
Disclosure of Interest P. Emery Grant/research support from: Bristol-Myers Squibb, Pfizer, MSD, AbbVie, UCB Pharma, Roche, Schering Plough, Novartis and Samsung, C. Bingham Consultant for: UCB Pharma, G.-R. Burmester Consultant for: AbbVie, MSD, Pfizer, Roche and UCB Pharma, V. Bykerk: None declared, D. Furst Grant/research support from: Abbott, Actelion, Amgen, Bristol-Myers Squibb, Gilead, GlaxoSmithKline, NIH, Novartis, Pfizer, Roche/Genentech and UCB Pharma, Consultant for: Abbott, Actelion, Amgen, Bristol-Myers Squibb, Biogen IDEC, Janssen, Gilead, GlaxoSmithKline, NIH, Novartis, Pfizer, Roche/Genentech and UCB Pharma, X. Mariette Grant/research support from: Pfizer, GlaxoSmithKline and Roche. Consulting fees from Bristol-Myers Squibb, GlaxoSmithKline, Pfizer, Roche, UCB Pharma and Sanofi-Aventis, D. van der Heijde Grant/research support from: AbbVie, Amgen, AstraZeneca, Augurex, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Centocor, Chugai, Covagen, Daiichi, Eli-Lilly, Galapagos, GlaxoSmithKline, Janssen, Merck, Novo-Nordisk, Otsuka, Pfizer, Roche, Sanofi-Aventis, UCB Pharma and Vertex, Consultant for: AbbVie, Amgen, AstraZeneca, Augurex, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Centocor, Chugai, Covagen, Daiichi, Eli-Lilly, Galapagos, GlaxoSmithKline, Janssen, Merck, Novo-Nordisk, Otsuka, Pfizer, Roche, Sanofi-Aventis, UCB Pharma and Vertex, Employee of: Director of Imaging at Rheumatology BV, R. van Vollenhoven Grant/research support from: AbbVie, BMS, GSK, Pfizer, Roche, UCB Pharma, Consultant for: AbbVie, Biotest, BMS, GSK, Janssen, Lilly, Merck, Pfizer, Roche, UCB Pharma, Vertex, B. VanLunen Employee of: UCB Pharma, C. Ecoffet Employee of: UCB Pharma, C. Cioffi Employee of: UCB Pharma, M. Weinblatt Grant/research support from: Amgen, Bristol-Myers Squibb, Crescendo Bioscience and UCB Pharma, Consultant for: AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Crescendo Bioscience, Lilly, MedImmune, Merck, Novartis, Pfizer, Roche and UCB Pharma