Article Text

Abstract
Background This study assessed the impact of simultaneous achievement of clinical, functional and structural efficacy, herein referred to as comprehensive disease control (CDC), on short-term and long-term work-related outcomes, health-related quality of life (HRQoL), pain and fatigue.
Methods Data were pooled from three randomised trials of adalimumab plus methotrexate for treatment of early-stage or late-stage rheumatoid arthritis (RA). CDC was defined as 28-joint Disease Activity Score using C reactive protein <2.6, Health Assessment Questionnaire <0.5 and change from baseline in modified Total Sharp Score ≤0.5. Changes in scores at weeks 26 and 52 for work-related outcomes, Short Form 36 (SF-36) physical (PCS) and mental component scores (MCS), a Visual Analogue Scale measuring pain (VAS-Pain) and Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) were compared between patient groups defined by achievement of CDC at week 26 using linear regression with adjustment for baseline scores.
Results Patients with RA who achieved CDC at week 26 (n=200) had significantly greater improvements in VAS-Pain (46.9 vs 26.9; p<0.0001), FACIT-F (13.3 vs 7.5; p<0.0001), SF-36 PCS (19.7 vs 8.9; p<0.0001) and SF-36 MCS (8.1 vs 5.0; p=0.0004) than those who did not (n=1267). Results were consistent at week 52 and among methotrexate-naive patients with early RA, methotrexate-experienced patients with late-stage RA and patients with inadequate response to methotrexate.
Conclusions Patients with RA who achieved CDC at week 26 had improved short-term and long-term HRQoL, pain, fatigue and work-related outcomes compared with patients who do not. These results demonstrate that the joint achievement of all CDC components provides meaningful benefits to patients.
Trial registration numbers DE019: NCT00195702, PREMIER: NCT00195702, OPTIMA: NCT00195702.
- Rheumatoid Arthritis
- Inflammation
- Patient perspective
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is characterised by progressive inflammation of the joints and leads to irreversible joint damage that reduces function and increases disability.1 ,2 Current treatment options have shown to reduce inflammation, slow or prevent joint damage and improve patient-related outcomes. As per the treat-to-target recommendations, the primary goal in the treatment of RA should be achieving the control of symptoms, prevention of structural damage, normalisation of function and social participation.3 In the European League Against Rheumatism (EULAR) 2013 guidelines, achievement of clinical, functional and structural efficacy is also the basis for treatment comparison. However, the impact of such achievement on patient outcomes has not been adequately and explicitly assessed.
While the achievement of all clinical, functional and structural efficacy is the ultimate goal for disease management, in real world practice, remission has been recommended as a key treatment target for adjusting therapy to optimise outcomes accordingly.3 Over the years, remission has been defined in several ways, but even with the recently more stringent American College of Rheumatology (ACR)-EULAR criteria, nearly 23% of the patients who achieved ACR-EULAR remission did not achieve the desired radiographic inhibition.4 It is, therefore, not guaranteed that remission target achievement alone would ensure functional and structural goal achievement. While remission could be the target for adjusting therapy, the goal of every treatment should be inhibition of structural damage and normalise function, in addition to symptom control.
In defining the three elements of the treatment goal, there has been a greater evolution in the definition of clinical remission relative to what is defined for normalised function based on Health Assessment Questionnaire disability index (HAQ-DI) and for structural non-progression based on modified Sharp score. Remission criteria derived from Disease Activity Score (DAS) and 28-joint Disease Activity Score (DAS28) have been the dominant treatment target in clinical practice in this evolution. Recently developed ACR-EULAR remission is so stringent that it is difficult to be achieved by most patients especially those with long-standing disease who actually constitute the majority of patients in clinical care. Hence, the EULAR 2013 guidelines recommended less stringent measures as a good alternative target for many patients who cannot attain stringent forms of remission.5 Given this, in the current study, we define clinical remission based on DAS28. A cut-off point of DAS28 using C reactive protein (DAS28(CRP)) <2.6 is an acceptable, as well as stringent enough, quantitative treatment target for the signs and symptoms of RA inflammation.6
Patient-reported outcomes (PROs) provide important assessments of functioning and well-being from the patient's perspective and may provide additional tangible impact for a patient, and thus be more sensitive to the effects of treatment than physician-assessed measures.7–10 In some cases, work limitations are important considerations in the treatment of RA given that the disease affects patients in their productive years.11 ,12 RA has also been noted to critically impact the health-related quality of life (HRQoL) of patients through the clinical manifestations of the disease and by socioeconomic, personal and environmental factors.7 ,13 Pain and fatigue are other important features of RA which are especially relevant from the patient perspective.8 ,14–16
In this study, we sought to quantify the impact of simultaneous achievement of clinical, functional and structural efficacy on work-related outcomes, HRQoL, pain and fatigue by pooling data from three randomised clinical trials of adalimumab for the treatment of RA among patients with both early-stage and late-stage disease.
Patients and methods
Patients
Data were drawn from three separate randomised controlled trials in RA: DE019 (NCT00195702), which enrolled patients with experienced RA (disease duration of at least 3 years with moderately to severely active RA despite a minimum of 3 months of treatment with methotrexate (MTX)); PREMIER (NCT00195663), which enrolled MTX-naive patients with early RA (disease duration <3 years) and OPTIMA (NCT00420927), which enrolled patients with early RA and included patients who failed to achieve stable low disease activity (LDA) (DAS28(CRP) <3.2 at weeks 22 and 26) with MTX. The design and primary results of the DE019, PREMIER and OPTIMA trials have been described elsewhere.17–20
A pooled intent-to-treat population included all patients from these trials who were randomised and received at least one dose of study drug. The present analysis includes all patients from DE019 and PREMIER. Due to the rerandomisation in the OPTIMA trial, only patients who failed to achieve LDA (DAS28(CRP) <3.2) with MTX during Period 1 of OPTIMA were included in the analysis. For these patients, the beginning of Period 2 was considered the baseline period. Patients with missing DAS28(CRP), HAQ-DI or change in modified total Sharp score (ΔmTSS) at baseline or week 26 were excluded from the present study.
The simultaneous achievement of stringent control of the signs and symptoms of inflammation, normal physical function and the absence of radiographic progression, herein referred as comprehensive disease control (CDC), was evaluated at week 26. Stringent control of the signs and symptoms of inflammation was assessed by DAS28(CRP) and defined as DAS28(CRP) <2.6.2 ,6 ,21 Normal physical function was assessed using the Disability Index of the HAQ-DI22 and defined as HAQ-DI <0.5.4 ,23 Radiographic progression was assessed using radiographs of the hands/wrists and feet scored using the mTSS method.24–26 Absence of radiographic progression was defined as a ≤0.5 unit change from baseline in mTSS.27 Patients who achieved all three components were considered to have achieved CDC (‘CDC achievers’), while patients who achieved either none or any one or two (partial achievers) of the three components were considered to have not achieved CDC (‘CDC non-achievers’).
Outcomes
Work-related outcomes were measured in DE032, the economic companion to PREMIER, and in OPTIMA. Work outcomes were analysed in each trial separately because of different definitions across the trials. Work outcomes in PREMIER/DE032 were measured using the Patient Health Economic Questionnaire (P-HEQ) and included the number of work days missed and the level at which work performance has been affected for employed patients with RA and homemakers separately. The level at which work performance has been affected was measured using a Visual Analogue Scale (VAS) scale ranging from 0 to 100.28 Work outcomes in OPTIMA were measured using the Work Productivity and Activity Impairment (WPAI) questionnaire29 and the RA-Work Instability Scale (RA-WIS).30 WPAI consists of six questions regarding the ability to work and perform regular activities during the past 7 days. WPAI evaluates absenteeism, presenteeism and work impairment among employed patients and activity impairment among all patients. RA-WIS is a 23-item questionnaire which quantifies ‘the state in which the consequences of a mismatch between an individual's functional abilities and the demands of his or her job can threaten continuing employment if they are not resolved’.30
HRQoL was measured using the Short Form 36 (SF-36) health survey. The SF-36 is a 36-item generic HRQoL measure to assess the patient’s view of his or her health consisting of two summary scales: physical (PCS) and mental component scores (MCS). For each component, a normalised summary score was calculated such that the average in the general population is 50 (with an SD of 10) using eight subdomains: Physical Functioning, Role-Physical, Bodily Pain and General Health for PCS, and Vitality, Social Functioning, Role-Emotional and Mental Health for MCS. Scores range from 0 to 100, with greater scores reflecting better health status.31–34 The minimal clinically important difference (MCID) for the SF-36 PCS and MCS is a 2.5-point increase from baseline.35 SF-36 information was not collected in the OPTIMA trial.
Pain was measured using a VAS ranging from no pain to worst pain imaginable, with a higher score indicating worse pain. The MCID for VAS-Pain was a 10-mm decrease from baseline.36 Fatigue was measured using the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), a symptom-specific scale validated for patients with RA. The 13-item subscale is self-administered using a 5-point Likert rating scale and ranges between 0 and 52 with higher values indicating less fatigue.37 The MCID for FACIT-Fatigue is a 4-point increase from baseline.32
Statistical analysis
Baseline characteristics were described for patients who achieved and did not achieve CDC at week 26. The change from baseline to week 26 for each outcome variable was compared between CDC achievers and non-achievers using linear regression adjusting for the baseline value of each outcome. Work outcomes measured using the P-HEQ were analysed in PREMIER only, while work outcomes measured using WPAI and RA-WIS were analysed in OPTIMA only. Similar analyses were performed to compare change from baseline to week 52. VAS-Pain and FACIT-F were analysed by pooling data from all three randomised clinical trials and in each trial separately. SF-36 PCS and SF-36 PCS were analysed by pooling DE019 and PREMIER because these HRQoL measures were not collected in OPTIMA. Separate analyses were conducted within the early RA (PREMIER), the MTX-failure (OPTIMA) and the experienced RA (DE019) populations. To gauge the incremental benefit of the simultaneous achievement of the three CDC components, the differences in SF-36 PCS, MCS, FACIT-F and VAS-Pain were compared between patients achieving all three components compared with achieving each component individually using a full interaction model adjusting for the baseline value of each outcome. To assess differences between CDC achievement and ACR-EULAR remission achievement, the differences in SF-36 PCS, MCS, FACIT-F and VAS-Pain were compared between patients achieving CDC compared with those achieving ACR-EULAR remission (Boolean-based definition4) but not CDC adjusting for the baseline value of each outcome.
Results
A total of 1467 patients were included in the pooled trial sample (493 (33.6%) from DE019, 661 (45.1%) from PREMIER and 313 (21.3%) from OPTIMA) of whom 200 (13.6%) achieved CDC. Overall, patients who achieved CDC at week 26 were younger, had lower mean DAS28(CRP), HAQ-DI, mTSS and VAS-Pain, and higher mean FACIT-F, SF-36 PCS and SF-36 MCS scores (table 1).
Patient characteristics of week 26 CDC achievers and non-achievers
Pooled RA population
After adjusting for the baseline value of the outcome, CDC at week 26 was associated with the following improvements in PROs at week 26: a 20.0 (95% CI 16.9 to 23.2) point improvement in change from baseline in VAS-Pain; a 5.8 (4.4 to 7.1) point improvement in FACIT-F; a 10.8 (9.1 to 12.4) point improvement in SF-36 PCS and a 3.1 (1.4 to 4.8) point improvement in SF-36 MCS. Further, after adjusting for the baseline value of the outcome, CDC at week 26 was associated with the following improvements in PROs at week 52: a 16.9 (13.5–20.2) point improvement in VAS-Pain; a 4.9 (3.5–6.4) point improvement in FACIT-F; a 9.3 (7.6–11.1) point improvement in SF-36 PCS and a 2.2 (0.4–3.9) point improvement in SF-36 MCS (table 2). All improvements were statistically significant. In addition, the differences in SF-36 PCS, VAS-Pain and FACIT-F exceeded their respective MCIDs at both week 26 and 52. The difference in SF-36 MCS only exceeded the MCID at week 26.
Comparison of patient-reported and work-related outcomes by week 26 CDC achievement*†
Early RA population
Among patients with early RA enrolled in PREMIER, CDC achievement was associated with statistically significant improvements in P-HEQ presenteeism at weeks 26 and 52 (table 2). Achievement of CDC at week 26 was also associated with statistically significant and clinically meaningful differences in SF-36 PCS, VAS-Pain and FACIT-F at both week 26 and 52 and statistically significant and clinically meaningful differences in SF-36 MCS at week 26 (figures 1 and 2).
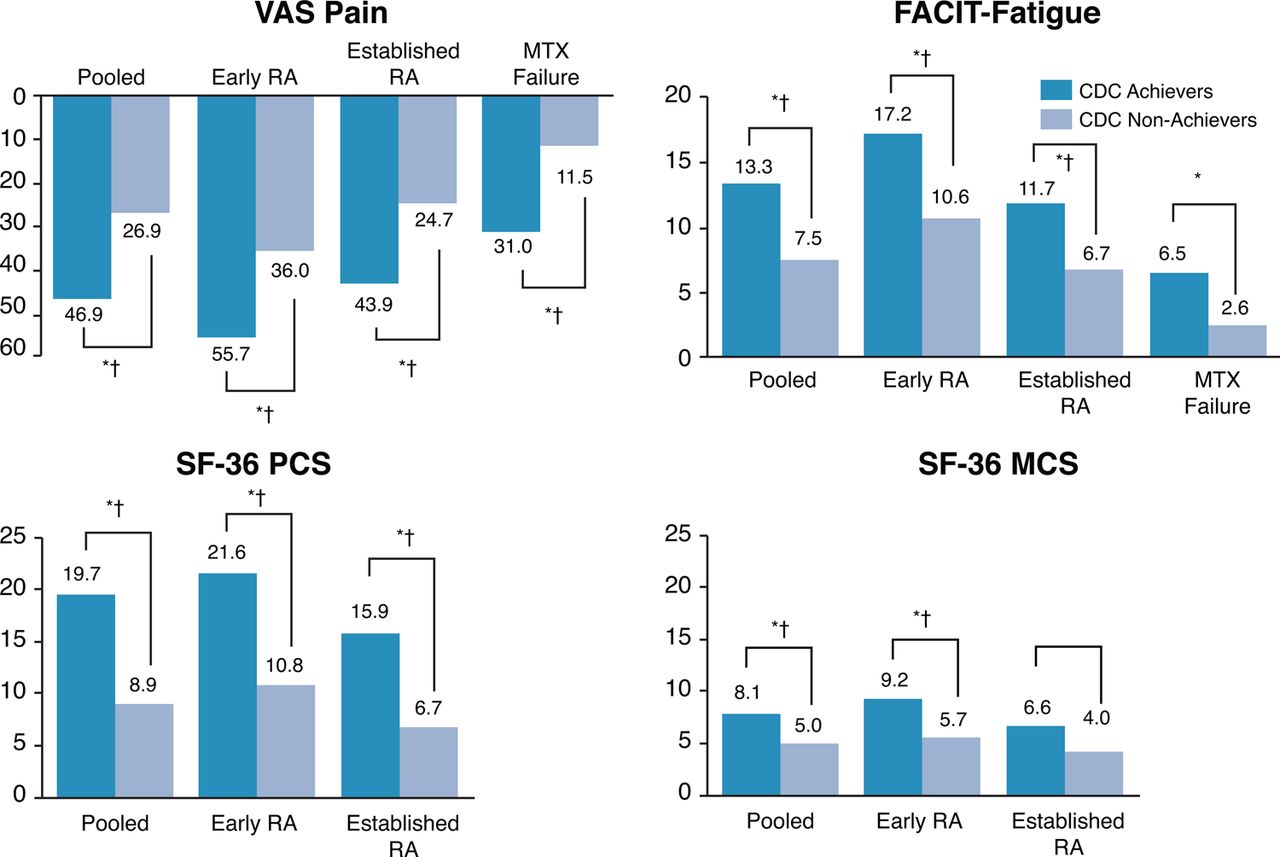
Comparison of patient-reported outcomes by CDC achievement and trial population at week 26.1 FACIT, Functional Assessment of Chronic Illness Therapy; SF-36, Short Form 36; VAS, Visual Analogue Scale; RA, rheumatoid arthritis; MCS, mental component score; PCS, physical component score; CDC, comprehensive disease control; MTX, methotrexate.

{kind=link}
{kind=link}
Comparison of patient-reported outcomes by CDC achievement and trial population at week 52.1 FACIT, Functional Assessment of Chronic Illness Therapy; SF-36, Short Form 36; VAS, Visual Analogue Scale; RA, rheumatoid arthritis; MCS, mental component score; PCS, physical component score; CDC, comprehensive disease control; MTX, methotrexate.
Early RA MTX-failure population
Among all patients with early RA enrolled in OPTIMA who failed to achieve LDA with MTX, achievement of CDC at week 26 was associated with statistically significant improvements in change in WPAI activity impairment, WPAI work impairment, WPAI presenteeism and RA-WIS at weeks 26 and 52 after adjusting for baseline values (table 2). Among all MTX-failure patients, achievement of CDC at week 26 was associated with statistically significant differences in VAS-Pain and FACIT-F at weeks 26 and 52 after adjusting for baseline values. The differences in VAS-Pain exceeded the MCID at both week 26 and 52 (figures 1 and 2).
Established RA population
Among patients with established RA enrolled in DE019, achievement of CDC at week 26 was associated with statistically significant improvements in change in SF-36 PCS, FACIT-F and VAS-Pain at weeks 26 and 52 after adjusting for the baseline scores (figures 1 and 2).
Incremental value of CDC
Compared with patients achieving DAS remission alone, CDC achievement was associated with statistically significant and clinically meaningful differences of 7.0 (4.0–10.0) and 6.9 (3.5–10.4) in SF-36 PCS at weeks 26 and 52, respectively. CDC achievement was also associated with a 9.0 (1.6–16.3) point decrease in VAS-Pain compared with DAS remission alone. When compared with patients achieving normal physical function alone, CDC achievement was associated with statistically significant differences of 4.0 (2.0–6.0) and 2.9 (0.6–5.2) in SF-36 PCS and 7.6 (3.1–12.1) and 5.5 (0.5–10.6) reductions in VAS-Pain at weeks 26 and 52, respectively. CDC achievement was associated with statistically significant and clinically meaningful improvements in SF-36 PCS, MCS, FACIT-F and VAS-Pain at both week 26 and 52 compared with patients with the absence of radiographic progression alone (table 3).
Change in patient-reported outcomes from baseline to week 26 and week 52 by week 26 CDC components achieved (DE019, PREMIER and OPTIMA)
Comparison with ACR-EULAR remission
There were no statistically significant differences in VAS-Pain, FACIT-Fatigue, SF-36 PCS and SF-36 MCS between patients achieving CDC and patients achieving ACR-EULAR remission but not CDC at weeks 26 and 52 (table 4).
Change in patient-reported outcomes from baseline to week 26 and week 52 by week 26 CDC/ACR-EULAR remission achievement (DE019, PREMIER and OPTIMA)
Discussion
Clinical, functional and structural efficacy outcomes are the three aspects against which therapies are evaluated in the disease management for RA. In additional, simultaneous achievement of all three is proposed as the long-term treatment goal with implied benefits on patients. While correlated, these three aspects have respective variations and each of them adds value while being achieved simultaneously. The purpose of this study is to assess the impact of such achievement, referred to as CDC, on short-term as well as long-term patient outcomes including fatigue, pain, work outcomes and general physical and mental health. CDC includes DAS remission of <2.6, normal physical function (as measured by HAQ-DI) and absence of radiographic progression (as measured by mTSS).
In the present study, CDC was associated with significant improvements in patient's work-related outcomes, HRQoL, pain and fatigue. These improvements were observed both at the time of CDC achievement and 26 weeks later. The improvements in HRQoL are especially pronounced, as patients who achieve CDC are 2.5 times more likely to have SF-36 MCS score greater than the general population norm and 9.8 times more likely to have SF-36 PCS greater than the general population norm at week 26. Similarly, CDC achievers are 2.3 times more likely to have SF-36 MCS score greater than the general population norm and 6.7 times more likely to have SF-36 PCS greater than the general population norm at week 52. These improvements are associated with reduced healthcare use and costs and reduced mortality,38 ,39 further demonstrating that CDC achievement is associated with broad and significant improvements in patient outcomes. Also, the differences between the CDC achievers and non-achievers for all the measured outcomes were greater than the clinically meaningful thresholds for each of the outcome. The simultaneous achievement of all three CDC domains was also demonstrated to be associated with significant improvements in physical function and pain compared with achieving the individual domains in isolation. This result suggests there may be an incremental benefit related to achieving all three components. An adjusted correlation analysis of the individual components showed that nearly 50%–55% of the variations in the outcomes at week 26 (SF-36 and VAS-Pain) were explained by improvements in DAS28 remission, 35%–47% by improvements in HAQ-DI score and 2%–9% by mTSS scores.
Current recommendations state that treatment of RA should focus on achieving clinical remission to inhibit progression of joint damage and improve physical function and quality of life.3 The ACR and EULAR also recognise the importance of remission for predicting improvement in physical function and halting radiographic progression. It is noted in the EULAR 2013 recommendation update that ACR-EULAR remission should serve as the optimal treatment target to be used in routine clinical practice, while LDA is a good alternative for the many patients who cannot attain remission. Within the pooled population in this study, a total of 94 patients experienced ACR-EULAR remission, of whom 65 (69.1%) also achieved CDC. The presence of radiographic progression was the most common reason for discordance (17 patients). There were no significant differences in SF-36 PCS, MCS, FACIT-F or VAS-Pain between patients achieving CDC and those achieving ACR-EULAR remission (but not CDC), although this analysis was limited by small sample size (table 4). Regardless of which treatment target is selected, the long-term goal remains to maximise long-term HRQoL through control of symptoms, prevention of structural damage, normalisation of function and social participation. Discussions around the simultaneous achievement of clinical, physical and structural efficacy can also engage patients and encourage patients to involve their observation around physical function.
This analysis has several strengths. First, we pooled data from three large RCTs of early RA, established RA and MTX non-responders and found that within trial, analyses were consistent with the results from the pooled data. So while patients with experienced disease may achieve CDC at a lower rate, there is no differential impact of CDC achievement on quality of life by RA duration. Further, improvements in PROs observed at 52 weeks were similar to those observed at 26 weeks, demonstrating that achievement of CDC may have a long-standing effect on quality of life.
This analysis has limitations. First, patient characteristics were not balanced between CDC achievers and non-achievers. However, adjustment for these factors may not account for all baseline differences between CDC achievers and non-achievers. An observed case analysis was performed, which led to 17% of patients being dropped from the analysis. However, imputation procedures require assumptions about the underlying missing data mechanism and may not be appropriate for this analysis. Last, not all outcomes, such as SF-36, were measured in all trials making it difficult to assess the full impact of CDC achievement on SF-36 in patients who were non-responders to MTX.
This post hoc analysis of three individual clinical trials demonstrated the benefits of CDC at the time of achievement and 6 months postachievement. This finding can be strengthened if supported by the results of a future prospective randomised controlled trial using CDC as a ranked secondary endpoint. Future research into whether the benefits of CDC are maintained over a longer-term is also warranted.
CDC achievement was associated with clinically meaningful improvements in work-related outcomes, HRQoL, pain and fatigue compared with those who did not achieve CDC. These results demonstrate that simultaneous improvement in all three RA domains can provide meaningful benefits to patients.
References
Footnotes
Handling editor Tore K Kvien
Contributors PE, AK and PM conceptualised the research and contributed to the interpretation of the data. YB and AG wrote the statistical analysis plan and analysed the data. AG, PE, AK, PM and YB contributed to the drafting of the paper and approved the final version. Significant contribution towards medical writing and analytical support was provided by Keith Betts, PhD, of Analysis Group; this support was funded by AbbVie. AbbVie sponsored the studies, participated in study design, data collection, analysis and interpretation, and in the writing, reviewing and approval of the final version.
Funding AbbVie funded the studies DE019 (NCT00195702), PREMIER (NCT00195663) and OPTIMA (NCT00420927), contributed to their design and was involved in the collection, analysis and interpretation of the data, and in the writing, review and approval of the manuscript.
Competing interests PE—Grant/research support: AbbVie, Pfizer, Novartis, BMS and Roche; Consultant for: AbbVie, Pfizer, MSD, UCB, Roche, Novartis and BMS. AK—Grant/research support: AbbVie, Amgen, Astra-Zeneca, BMS, Celgene, Centocor-Janssen, Pfizer, Roche and UCB; Consultant for: AbbVie, Amgen, Astra-Zeneca, BMS, Celgene, Centocor-Janssen, Pfizer, Roche and UCB. AG—Shareholder of: AbbVie; Employee of: AbbVie. YB—Shareholder of: AbbVie; Employee of: AbbVie. PM—Shareholder of: AbbVie; Employee of: AbbVie.
Provenance and peer review Not commissioned; externally peer reviewed.