Article Text

Abstract
Background Abatacept (ABT), a selective co-stimulation modulator, is the first in a new class of biologic agents for the treatment of rheumatoid arthritis (RA) that inhibits T cell activation by binding to CD80/86, and modulating its interaction with CD28. The AMPLE trial demonstrated that clinical efficacy of ABT was equivalent to adalimumab [1]. However, some physicians make assertions that the treatment response of ABT seems to be slower than other class biological DMARDs and we should wait longer periods before deciding whether to continue ABT.
Objectives We studied the appropriate periods for deciding to continue or discontinue ABT, by using data from the Japanese multicenter registry system for RA patients using biological DMARDs.
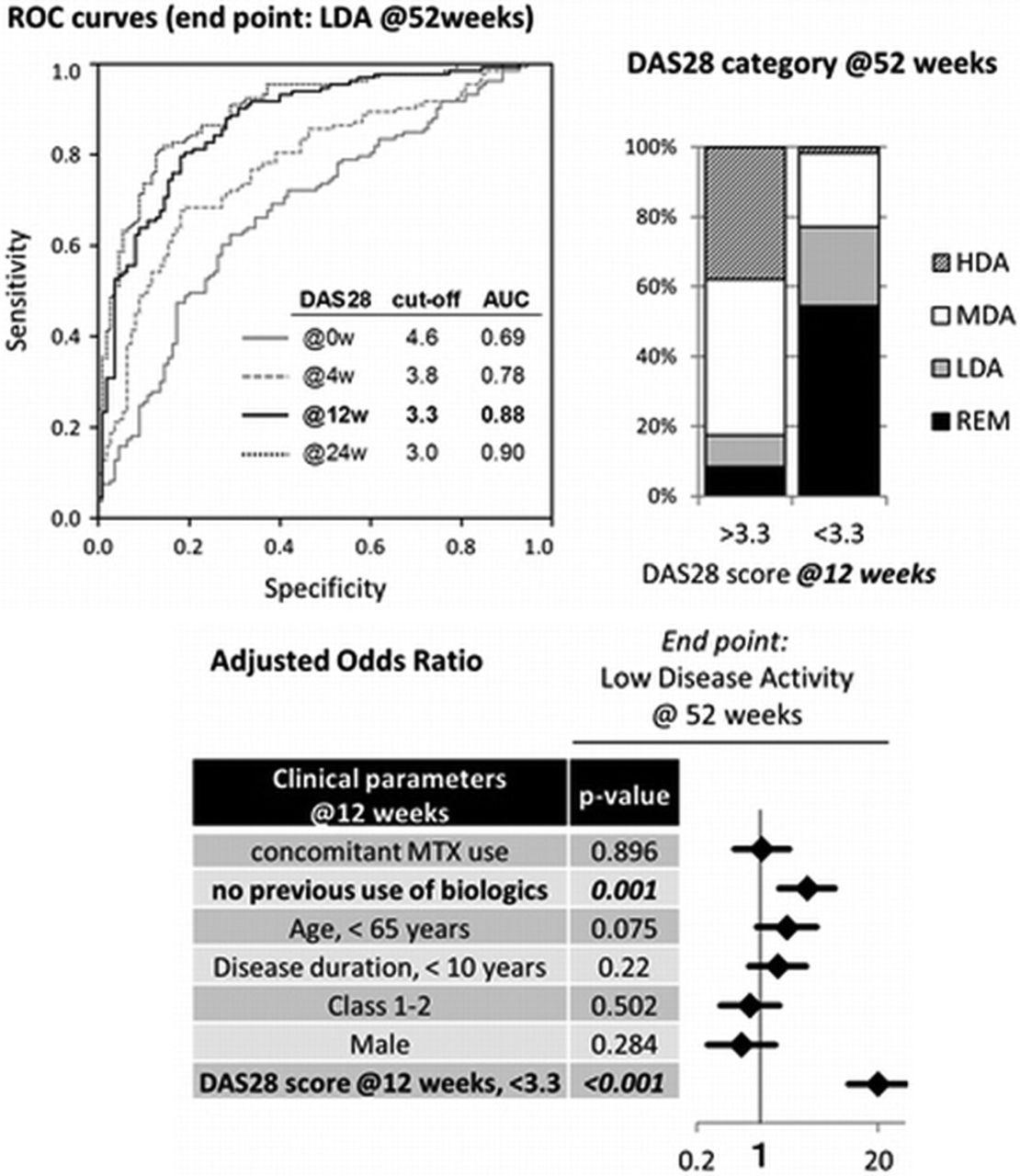
Methods All RA patients who underwent ABT treatment for at least 52 weeks (n=254) in Nagoya University Hospital and 12 other institutes (Tsurumai Biologics Communication Registry Study Group [2]) were enrolled in this study. Demographic data and the following parameters of disease activity were collected; tender joint count (TJC) and swollen joint count (SJC) on 28 joints, patient global assessment (VAS), ESR, and serum CRP and MMP-3 levels at baseline, 4, 12, 24, and 52 weeks. The last observation carried forward (LOCF) method was used in each analysis. We used a conventional receiver-operating-characteristic (ROC) curve to analyze DAS28 scores at each time point in order to determine the cutoff points that yielded the highest combined sensitivity and specificity with respect to distinguish patients achieved low disease activity (LDA, DAS28-CRP <2.3) at 52 weeks from those did not.
Results In the baseline characteristic data, mean age was 64.5 years, mean disease duration was 11.3 years, and proportion of patients with previous biological DMARDs history was 48.0% and with concomitant MTX usage was 48.8%. We analyzed DAS28 scores at baseline, 4, 12, and 24 weeks. As shown in Fig. 1 left panel, area-under-curve (AUC) was lowest in baseline DAS28 score and highest in 12 and 24 weeks. We chose the shorter time point, 12 weeks, for further study. The cutoff point of DAS28 score at 12 weeks that gave the maximal sensitivity (81%) and specificity (81%) was 3.3. Seventy seven percent of the patients with lower than 3.3 of DAS28-CRP at 12 weeks achieved LDA at 52 weeks (Fig. 1 right panel). Logistic regression analysis identified the previous biological DMARDs history and DAS28-CRP score (<3.3 at 12 weeks) as independent predictors of LDA at 52 weeks (Fig. 1 bottom panel). Adjusted Odds Ratio (OR) of DAS28-CRP score was much higher than that of the previous biological DMARDs history.

{kind=link}
Conclusions According to the difference of AUC score, 4 weeks would be too short and 12 weeks would be long enough to predict low disease activity at 52 weeks in the RA patients treated with ABT. Since we usually decide whether to continue anti-TNF agents at 12 weeks, the treatment response of ABT seemed to be equivalent to that of anti-TNF agents as shown in the AMPLE trial. We would suggest that we can decide to discontinue ABT and switch to other agents if the treatment response is insufficient at 12 weeks.
References
Arthritis Rheum. 2013;65:28.
Mod Rheumatol. 2013;23:904.
Disclosure of Interest None declared
DOI 10.1136/annrheumdis-2014-eular.2349