Article Text

Abstract
Background The Ankylosing Spondylitis Disease Activity Score (ASDAS) is a new Assessment of SpondyloArthritis international Society (ASAS) and Outcomes in Rheumatology (OMERACT)-endorsed measure of disease activity in axial spondyloarthritis (SpA). The ASDAS preferred formula includes C-reactive protein (CRP) and the alternative formula includes erythrocyte sedimentation rate (ESR). It was recommended that when conventional CRP values are below the threshold of detection, half of the threshold value should be used (eg, if the limit of detection is 5 mg/l, a value of 2.5 should be used).[1] This recommendation requires additional testing and validation in independent cohorts. Furthermore, the agreement between ASDAS-CRP and ASDAS-ESR requires further investigation.
Objectives Our primary aim was to investigate the best method to calculate ASDAS-CRP when the conventional CRP value is below the threshold of detection. Our secondary aim was to assess the level of agreement between ASDAS-CRP and ASDAS-ESR.
Methods Baseline data from the Devenir des Spondylarthropathies Indifférenciées Récentes (DESIR) cohort was used. Two hundred and sixty patients fulfilling the ASAS classification criteria for axial SpA with a conventional CRP value below the threshold of detection (5 mg/l) were selected. High sensitivity CRP (hsCRP) was measured by particle-enhanced immunoturbidimetry and ASDAS-hsCRP was used as the gold-standard. ASDAS-CRP was calculated using three different options for the conventional CRP value: 1) the threshold value (ASDAS-CRP(5)), 2) half of the threshold value (ASDAS-CRP(2.5)), and 3) zero value (ASDAS-CRP(0)). ASDAS-ESR was also calculated. The intraclass correlation coefficient (ICC) and the Bland-Altman technique were used to investigate agreement between formulae. ASDAS disease activity states were derived and agreement was studied using the weighted kappa statistics.
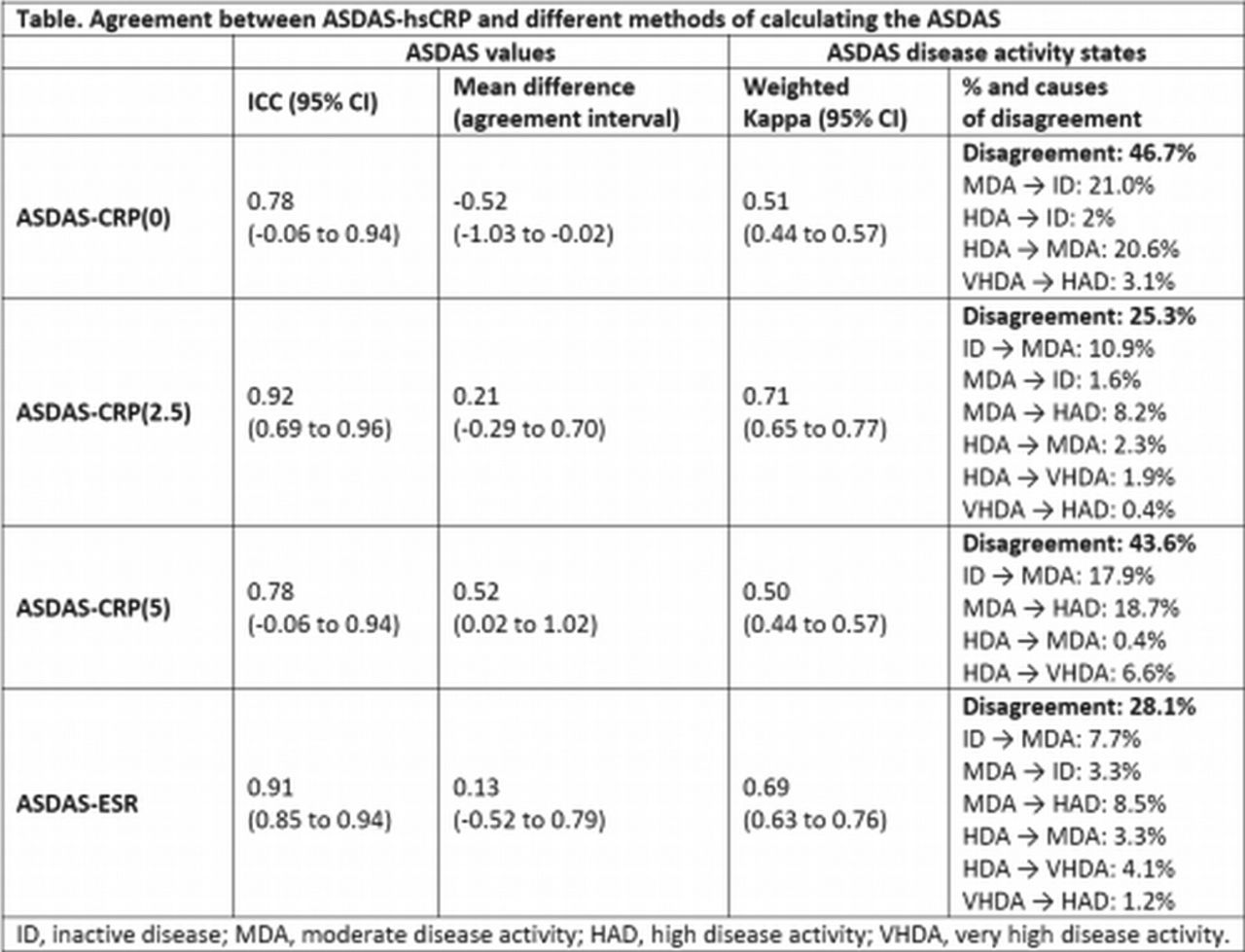
Results ASDAS-hsCRP and ASDAS-ESR were available in 257 and 246 patients, respectively. Agreement between ASDAS-hsCRP and ASDAS-CRP(2.5) was good, while only moderate with ASDAS-CRP(0) and -CRP(5). Agreement between ASDAS-hsCRP and ASDAS-ESR was also good (table). When using ASDAS-CRP(2.5), this classified a slightly higher degree of disease activity than ASDAS-hsCRP but disagreement was mainly in lower disease activity states (inactive disease – moderate disease activity), a shift that has less therapeutic implications than the shift between moderate and high disease activity (table).
{kind=link}
Conclusions When conventional CRP values are below the threshold of detection and hsCRP is not available, half of the threshold value of the CRP should be used to calculate ASDAS-CRP. There is also good agreement between ASDAS-hsCRP and ASDAS-ESR; however, formulae are not interchangeable.
References
-
Machado et al. Ann Rheum Dis. 2011 Jan;70(1):47-53.
Acknowledgements An unrestricted grant from Wyeth Pharmaceuticals was allocated for the first 5 years of the follow-up of the recruited patients.
Disclosure of Interest None declared
DOI 10.1136/annrheumdis-2014-eular.1095