Article Text

Abstract
Background Ustekinumab – a fully human monoclonal antibody against interleukins 12 and 23 – has been shown to be effective in reduction of symptoms of active ankylosing spondylitis (AS) in a proof-of-concept study (TOPAS) [1].
Objectives The purpose of the current work was to investigate the impact of ustekinumab on active inflammation and post-inflammatory structural changes in the sacroiliac joints (SIJ) and in the spine as detected by magnetic resonance imaging in the TOPAS study.
Methods In the TOPAS study, ustekinumab in a dose of 90 mg was administered subcutaneously at baseline, week 4 and week 16 in 20 patients with active AS. Eligible patients were required to have a diagnosis of AS according to the modified New York criteria and an active disease defined as a BASDAI score of ≥4 despite previous NSAIDs treatment. MRI of the SIJ and of the spine (STIR and T1-weighted sequences) was performed at baseline and at week 24. Images were scored according to the Berlin scoring system for active inflammation and for chronic changes [2], including a detailed fatty degeneration score for SIJ, independently by two trained readers in a concealed and randomly selected order, blinded for all clinical data.
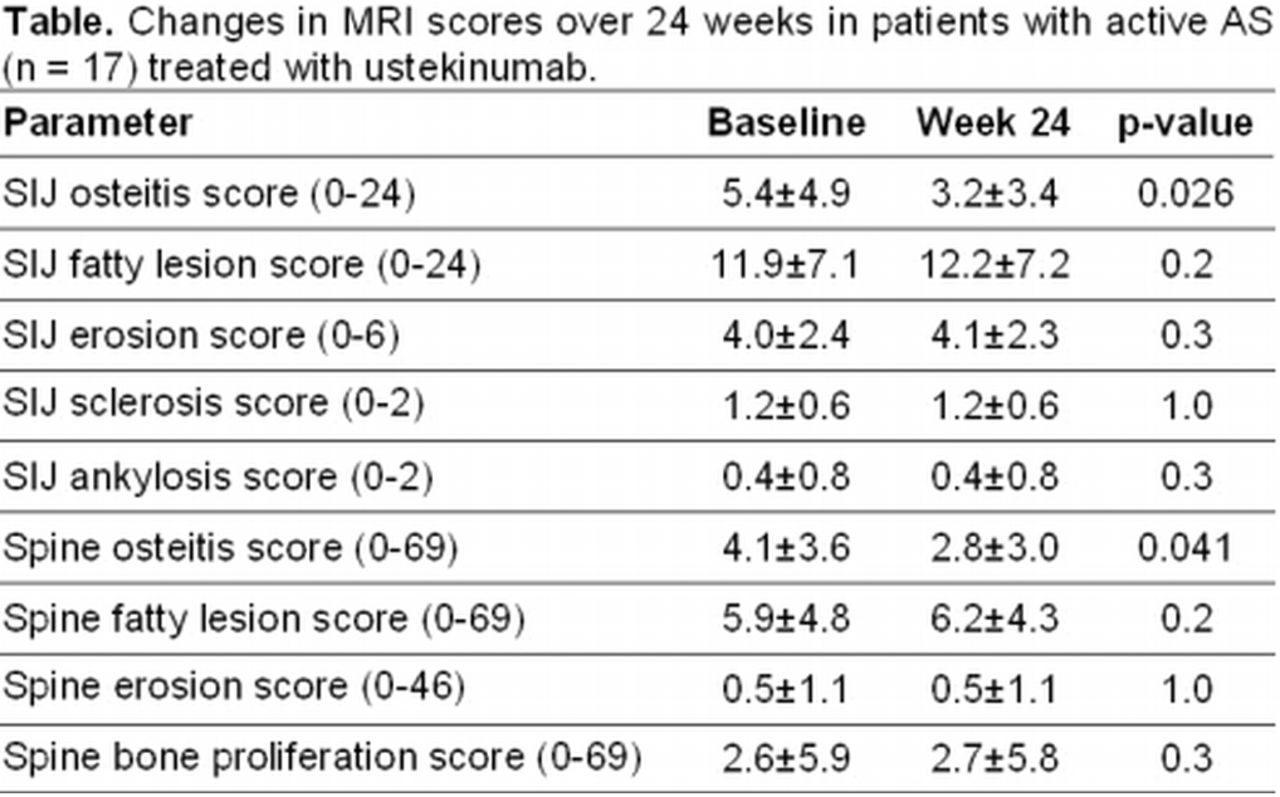
Results Complete MRI sets (baseline and follow-up) were available in 17 patients (13 ASAS40 responders and 4 non-responders; in 3 ASAS40 non-responders no follow-up MRIs were available). There was a significant reduction of active inflammation on MRI at week 24 as compared to baseline both in the SIJ (osteitis change score -2.2±3.8 corresponding to 41% reduction) and in the spine (osteitis change score -1.2±2.3 corresponding to 31% reduction) – table. Reduction of active inflammation after 24 weeks was more prominent and statistically significant in patients with clinical response (ASAS40): osteitis change score in the SIJ was -3.1±3.8 in responders as compared to +0.6±1.3 in non-responders, p=0.015; similarly, osteitis change score in the spine was -1.9±1.9 in responders as compared to +1.0±2.4 in non-responders, p=0.023. Notably, clinical response (ASAS40) to ustekinumab was associated with higher level of inflammation at baseline in the SIJ (osteitis score 6.7±4.9 in responders vs. 2.0±1.7 in non-responders, p=0.030), and in the spine (4.9±3.6 in responders vs. 3.6±4.1 in non-responders, p=0.2).
There were no substantial changes in the scores for post-inflammatory lesions including fatty lesions in the entire group – table. However, the SIJ fatty lesion score increased significantly in patients with improvement of SIJ osteitis score by at least one point at week 24 (n=11): +0.8±1.1 vs.-0.4±0.8 in patients without osteitis improvements, p=0.022.
{kind=link}
Conclusions Ustekinumab effectively reduced active inflammation in the axial skeleton as detected by MRI in patients with AS after 24 weeks of treatment. There was a clear correlation between clinical and MRI responses. Higher level of active inflammation at baseline was associated with good clinical response.
References
-
Poddubnyy D, et al. Ann Rheum Dis 2014 Jan 3 [Epub ahead of print].
-
Althoff CE, et al. Ann Rheum Dis. 2013;72:967-73.
Acknowledgements Grant from Janssen-Cilag.
Disclosure of Interest D. Poddubnyy Speakers bureau: Abbvie, Merck Sharp & Dohme, Pfizer and UCB, K.-G. Hermann Speakers bureau: Abbvie, Janssen Research & Development, MSD, J. Callhoff: None declared, J. Listing: None declared, J. Sieper Grant/research support: Merck Sharp & Dohme, Pfizer, Abbvie and Janssen-Cilag, Consultant for: Abbvie, Hoffmann-La Roche, Eli Lilly and Company, Merck Sharp & Dohme, Pfizer, Abbvie and Novartis, Speakers bureau: Abbvie, Merck Sharp & Dohme, Pfizer and UCB
DOI 10.1136/annrheumdis-2014-eular.1216