Article Text

Abstract
Background Sweden has become an increasingly multicultural society over the past twenty years, about 15 % of people living in Sweden are born outside Sweden. Care providers see patients from all over the world on a daily basis and despite the fact that both parties do their best to get their message across in the medical consultation, misunderstandings can still occur. A combination of a different ethnic background and a rheumatic disease leads to increased disability problems. And those who had been diagnosed may very well be at a disadvantage in their contacts with the Health Service and other authorities. The Swedish Rheumatism Association decided 2009 to start a project “Be Welcome” together with The Swedish Society for Rheumatology and The Swedish Association of Health Professionals. The purpose of the project was” To develop and test tools and methods that facilitate the medical consultation between the Doctor/nurse and patient born outside Scandinavia with rheumatic disease and long-term pain.
Objectives People with different ethnic backgrounds and rheumatic disease will have the samne access to health care of high quality as the rest of the population.
Methods We used focusgroup discussions and in-depth interviews about the medical consultation. Ten focusgroup discussions and nine in-depth interviews were conducted with patients and careproviders at three health-care units and four groups of women born in other countries. Following questions were asked: What expectations did you have before the meeting with the care provider/patient? Did you get answers to your issues? What was positive/less positive in the meeting? What responsibility do you have as patient/care provider for the meeting to succeed? These discussions and interviews were taped, transcribed and analyzed.
Results We identified several factors that facilitate or impede the medical consultation. The amount of time allocated for the consultation was a significant factor in ensuring that the consultation was satisfactory, as was the care provider’s knowledge of and access to supervision for handling this patient group. Patient´s language skills, their expectations in relation to Swedish healthcare, and perceptions of symptoms and treatment that may differ from the careprovider´s perception were factors that could generate feelings of powerless and frustration. This became the basis of the designed model. We called the model “Bredängsmodellen” after the health care clinic we collaborated with. “When pain speaks different languages” is the title of a booklet that describes how to handle a medical consultation with a patient not born in Sweden with rheumatic diagnosis and pain. It is based on the result from focusgroups and meetings with experts during this three year the project has continued. We have also produced a material for the patient to study before the medical consultation called “Pain”.

{kind=link}
Conclusions Our tools and booklets can easily be used in health care clinics and we know that there is a high demand in Sweden for knowledge of what we have achieved. Because of that we have initiated a collaboration with Rheuma Utveckling AB to educate care providers about these things and inform our members to strengthen other patients.
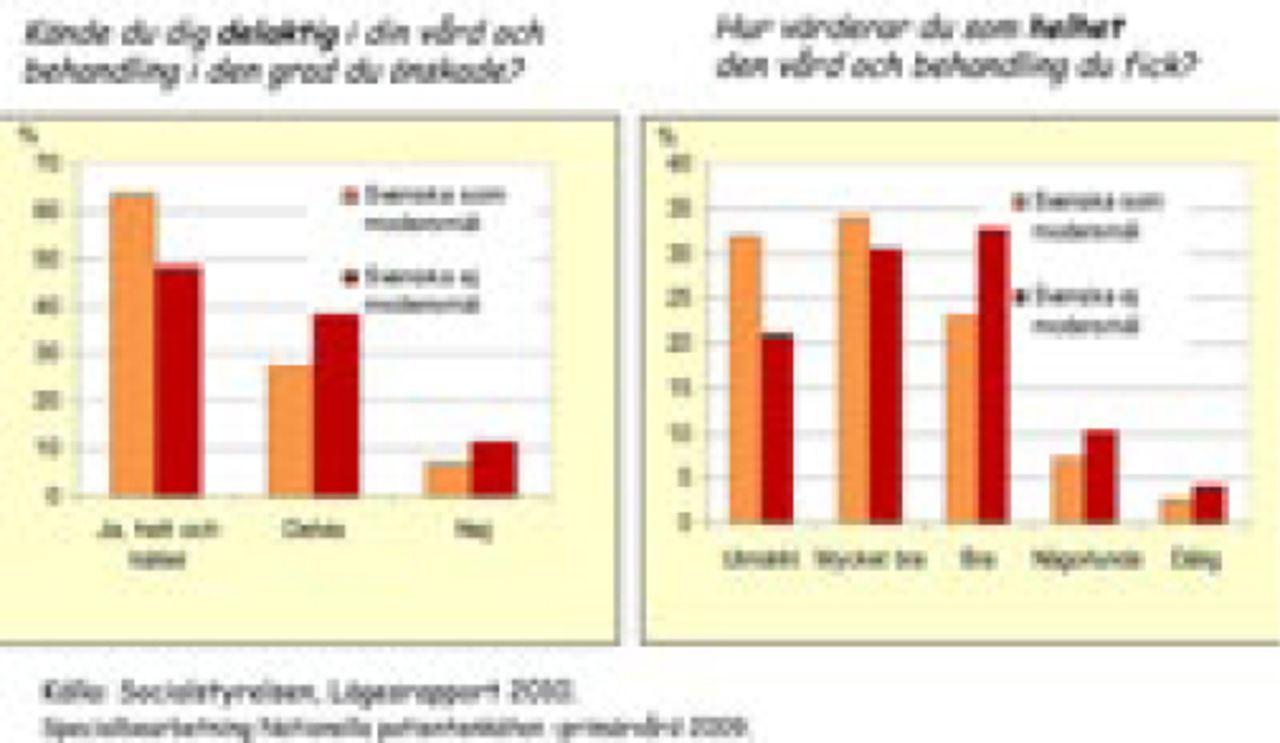
References Questions from left to right “Did you feel involved in the care and the treatment, “What do you think about the care and treatment you received”
Disclosure of Interest None Declared