Article Text

Abstract
Objective To determine the effect of chondroitin sulphate (CS) treatment on cartilage volume loss, subchondral bone marrow lesions (BML), synovitis and disease symptoms in patients with knee osteoarthritis (OA).
Methods In this pilot multicentre, randomised, double-blind, controlled trial in primary knee OA, 69 patients with clinical signs of synovitis were randomised to receive CS 800 mg or placebo once daily for 6 months followed by an open-label phase of 6 months in which patients in both groups received CS 800 mg once daily. Cartilage volume and BML were assessed by MRI at baseline and at 6 and 12 months; synovial membrane thickness was assessed at baseline and at 6 months.
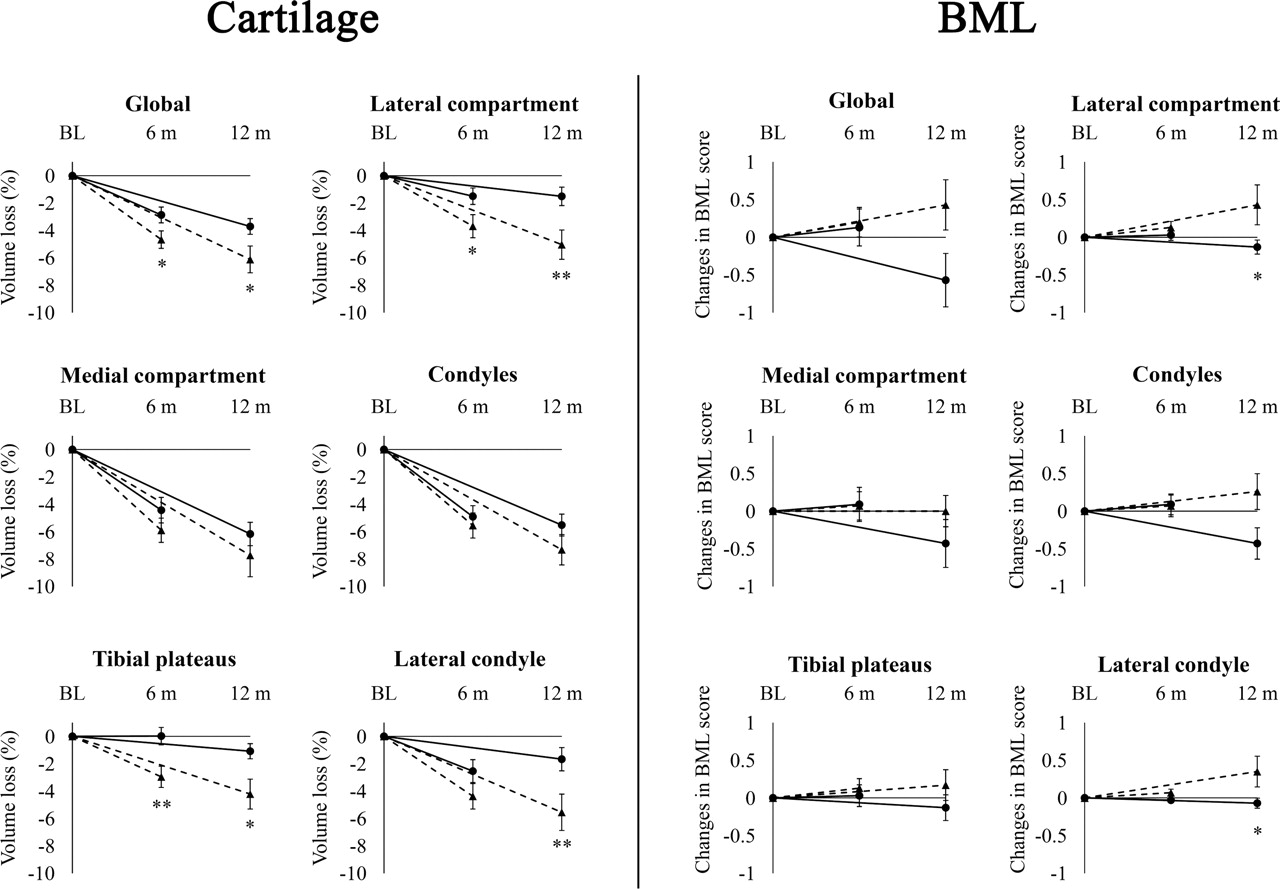
Results The CS group showed significantly less cartilage volume loss than the placebo group as early as 6 months for the global knee (p=0.030), lateral compartment (p=0.015) and tibial plateaus (p=0.002), with significance persisting at 12 months. Significantly lower BML scores were found for the CS group at 12 months in the lateral compartment (p=0.035) and the lateral femoral condyle (p=0.044). Disease symptoms were similar between the two groups.
Conclusion CS treatment significantly reduced the cartilage volume loss in knee OA starting at 6 months of treatment, and BML at 12 months. These findings suggest a joint structure protective effect of CS and provide new in vivo information on its mode of action in knee OA.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Of all musculoskeletal conditions, osteoarthritis (OA) has the highest prevalence, affecting a significant percentage of the ageing population.1,–,3 Management of OA requires a long-standing combination of pharmacological and non-pharmacological treatment modalities to relieve pain and to maintain joint mobility in daily life.4 Many attempts have therefore been made during the past decades to find treatments that can not only offer pain management, but also alter the course of the disease with the lowest possible risk of adverse events. Only a few medications have been recognised by clinical trials to potentially influence the course of OA beneficially: these include chondroitin sulphate (CS),5,–,8 glucosamine,9,–,11 diacerein,12 doxycycline13 and licofelone.14 However, all previous disease-modifying OA drug (DMOAD) studies by other groups have used conventional x-rays, which, although recognised by the authorities, might not have fully explored the drugs' protective effect as this technique allows for only an indirect assessment of the cartilage. Recent advances in MRI have enabled investigators to quantitatively and reliably assess cartilage thickness and volume, as well as the other joint structural changes occurring in the subchondral bone, menisci and synovium.15,–,22 The usefulness of MRI technology in the context of clinical trials exploring DMOAD effects has recently been demonstrated.14 23
CS belongs to the glycosaminoglycans and is a major component of articular cartilage. On OA joint tissues, CS has been shown to modify the chondrocyte death process, to improve the anabolic/catabolic balance of the extracellular cartilage matrix, to reduce some pro-inflammatory and catabolic factors, and to reduce the resorptive properties of subchondral bone osteoblasts.24,–,35 Moreover, meta-analyses of randomised placebo-controlled trials in knee OA patients have demonstrated the efficacy of CS to relieve OA joint pain.36,–,38 CS at a dose of 800 mg orally once daily has been shown to slow significantly the rate of joint space narrowing (JSN) over a period of 2 years in patients with symptomatic radiographic knee OA.7 8 39 40 The aim of this study was to confirm the findings from x-ray-based trials on the effect of CS on cartilage volume loss in knee OA patients, yet at a much earlier time period by using MRI, and to evaluate the effect of treatment on subchondral bone lesions and synovitis severity.
Patients and methods
Study design
The present pilot study is a National Institutes of Health (NIH)-registered (NCT00604539) multicentre, randomised, double-blind, controlled trial comparing CS with placebo in patients with primary knee OA. The double-blind phase was of 6 months duration, followed by an open-label phase of 6 months of CS treatment for both groups. The study was conducted from February 2008 to October 2009.
Patient selection
Seventy patients of both sexes between 40 and 80 years of age were recruited from outpatient rheumatology clinics in the province of Québec, Canada. Inclusion criteria were primary OA of the knee diagnosed according to the clinical and radiological criteria of the American College of Rheumatology (ACR)41 with clinical signs of synovitis (warmth, swelling or effusion), a disease severity grade 2–3 based on the Kellgren–Lawrence radiographic system,42 a minimal medial joint space width (JSW) of 2 mm on standing knee x-ray, and a visual analogue scale (VAS) pain index of at least 40 mm while walking. Concomitant femoropatellar OA was not quantified on x-ray. Participants were required to have no significant laboratory abnormalities. If both knees were affected by OA, the knee with the more pronounced symptoms was selected if within inclusion criteria.
Exclusion criteria were the presence of another rheumatic condition leading to secondary OA (such as rheumatoid arthritis or calcium pyrophosphate dehydrate deposition disease), allergy to CS, contraindications to MRI, progressive serious medical conditions (such as cancer, AIDS or end-stage renal disease), impossibility of participating for the total duration of the study and attending the visits, as well as inability to give informed consent. Patients were also excluded if they were currently, or were within the 3 months prior to inclusion, being treated with corticosteroids, indomethacin, glucosamine, CS or radioactive synovectomy, or within the 6 months preceding inclusion, intra-articular treatment with hyaluronic acid.
Patients were randomly assigned to receive either CS 800 mg (two capsules of 400 mg each; Condrosan, CS Bio-Active; Bioibérica S.A., Barcelona, Spain) or placebo once daily for the first 6 months (double-blind phase) followed by 6 months of treatment with 800 mg CS once daily for both groups (open-label phase). Subjects started study medication at baseline visit according to the randomisation. Condrosan is a prescription drug containing highly purified chondroitins 4- and 6-sulphate of bovine origin in a concentration of not less than 98%. It has an average molecular weight of ∼15–16 kDa, and an intrinsic viscosity of ∼0.02–0.06 m3/kg. This product has been approved as a prescription treatment for OA in many European countries.
Prior and concomitant treatment
Treatment with medication for osteoporosis at baseline was continued, as were non-steroidal anti-inflammatory drugs (NSAIDs), in an unmodified manner for the entire duration of the study if so wished. The medications and other treatments in use for intercurrent illnesses were recorded at the baseline visit and during the study whenever these treatments were modified.
Rescue medication
Paracetamol up to 3 g/day was allowed as a rescue pain medication. During the open-label phase (from month 6 to 12) NSAIDs were also allowed when needed. The treatment had to be interrupted 24 h before all follow-up visits.
Blinding
The investigators, subjects and sponsors were blinded to the allocated treatment for the first 6 months. Through central randomisation, sealed coded tamper-proof envelopes, specifying the treatment group for each study drug kit number, were provided to each centre. The envelopes were to be opened only in the event of an emergency.
Treatment compliance
The number of tablets of the study drug taken was calculated from the drug dispensation log. The compliance index was calculated as the percentage of the rated drug doses taken between the date of dispensation and the date of return of the study drugs. To remain in the study, a global compliance index of ≥75% was mandatory.
Study schedule
Patients had a screening visit 7–14 days prior to baseline MRI including physical examination for joint swelling or effusion, x-ray and blood samples for routine laboratory tests to assess eligibility. A follow-up physical examination was performed at 3, 6 and 12 months. Patients were contacted every 45 days to report possible adverse events.
Outcome measures
Knee MRI acquisitions
MRI was performed at baseline and at 6 and 12 months on 1.5 T scanners (Siemens, Erlangen, Germany; and General Electric, Milwaukee, Wisconsin, USA) using a standard knee coil. The sequence acquisitions were as previously described14 15 43 (see online supplementary text).
Cartilage volume
Cartilage volume was measured by two trained readers (J Thériault and A Pelletier) using the computer program Cartiscope (ArthroVision, Montreal, Canada) as previously described.43 44 The readers were blinded to treatment and to MRI examination time points except for baseline. The change in knee cartilage volume was obtained by subtracting the follow-up volume from the initial (baseline) volume. The change in cartilage volume over time was calculated for the entire knee (global, comprising condyles plus tibial plateaus) and subregions including the condyles, tibial plateaus, the medial and lateral compartments (condyle plus tibial plateau), the medial and lateral condyle and tibial plateau, and the trochlea.16 45 The trochlea corresponds to the area of the femoral cartilage in contact with the patella.16 The patellar cartilage volume was not assessed. The reproducibility of the method has previously been demonstrated to be excellent.43
Synovial membrane thickness
Synovial membrane imaging was acquired as previously described21 (see online supplementary text). The extent of synovitis was assessed by measuring its thickness in mm in four regions of interest: the medial and lateral articular recess and the medial and lateral border of the suprapatellar bursa.21
Bone marrow lesions
Assessment of bone marrow lesions (BML) was performed in the same MRI sequences used for the cartilage assessment as previously described.46 The extent of the BML was assessed for the global knee and the subregions using the following scale: 0 = absence, 1 = <25%, 2 = 25–50%, and 3 = >50% of the surface of the respective region regardless of the presence of additional smaller lesions. Reliability of the scoring system for subchondral bone changes was found to be excellent.46
Symptoms
Pain, function and stiffness were assessed at baseline and at 1.5, 3, 6 and 12 months using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire and the VAS for pain. The impact on quality of life was also assessed at baseline and at 3, 6 and 12 months using the Short Form 36 General Health (SF-36) questionnaire.
Statistical analysis
Descriptive statistics were performed for all variables in the study. Measures of central tendency (mean, median) and dispersion (SD) were performed for all continuous variables and a proportion calculated for categorical variables.
p Values were assessed by analysis of covariance (ANCOVA) for which the dependent variable was the cartilage volume at 6 and 12 months, and the independent variables were the cartilage volume at baseline and the treatment. Adjustment was made for age and concomitant treatment with bisphosphonates, which could have had an influence on the subchondral bone. BML scores were assessed by the non-parametrical two-sided Mann–Whitney U test. For cartilage and BML, differences between the two groups were assessed for the global knee as well as the subregions. Comparison of synovial membrane thickness and pain levels between the two groups was assessed by analysis of variance (ANOVA) and joint swelling by Fisher's exact test. The analyses on the according-to-protocol population were done separately for the double-blind phase (0–6 months) and for the additional open-label phase (0–12 months). A p value less than 5% was considered statistically significant.
Endpoints
This study focused on the main structural changes observed in the synovial membrane (primary endpoint), cartilage and bone, as well as the pain levels (co-endpoints).
Results
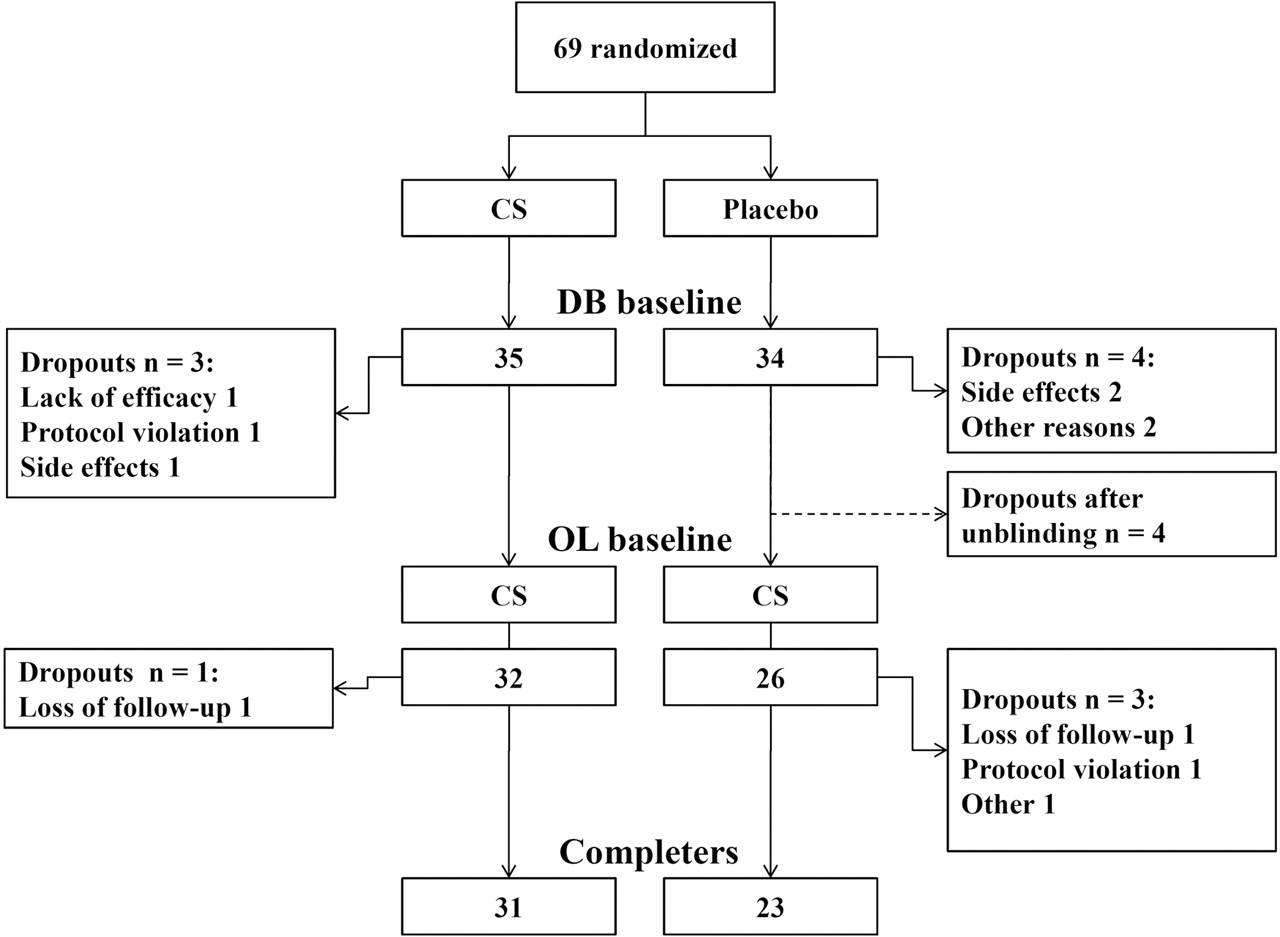
Seventy patients were enrolled in the study; 69 were included as one patient was found not to meet the eligibility criteria after enrolment. Sixty-two (88.6%) patients completed the double-blind phase of the study. Fifty-eight patients continued the study and entered the open-label phase, 54 (93.1%) of whom completed the study (figure 1). Fifty-four (78%) patients completed both phases.

Patient disposition. CS, chondroitin sulphate; DB, double-blind; OL, open-label.
Baseline characteristics
The baseline characteristics (table 1) were similarly distributed between the two treatment groups with the exception that patients in the CS group had a younger mean age.
Baseline characteristics
Cartilage volume
The data (table 2 and figure 2) revealed that patients in the CS group compared with those in the placebo group experienced a significant reduction in cartilage volume loss in the global knee at 6 months (p=0.030) that persisted at 12 months (p=0.021). A similar significant reduction was seen at both 6 and 12 months in the lateral compartment (p=0.015 and p=0.004, respectively) and the tibial plateaus (p=0.002 and p=0.017, respectively). Moreover, the reduction in both the lateral and medial tibial plateau was statistically different at 6 months (p=0.018 and p=0.016, respectively), with a trend at 12 months (p=0.068 and p=0.052, respectively). The lateral condyle also demonstrated a trend towards a reduction at 6 months (p=0.062) and a significant difference at 12 months (p=0.006). No difference was seen in the trochlea (table 2). After correction for age and concomitant osteoporosis treatment the results remained unchanged with the exception of the global knee with age (p=0.052) and the lateral and medial tibial plateau, which became statistically significant when adjusted for the treatment with bisphosphonates (table 2).
{kind=link}
{kind=link}
Cartilage volume loss in percentage and changes in bone marrow lesions (BML) score over time compared with baseline (0–6 months and 0–12 months). Solid line, chondroitin sulphate (CS) group; dotted line, placebo group. p Values of the corresponding subregions were assessed by analysis of covariance (ANCOVA) for the cartilage volume (where the dependent variable was the cartilage volume at 6 and 12 months and the independent variables were the cartilage volume at baseline and the treatment) and by the non-parametric Mann–Whitney U test for the BML scores. *p<0.05,**p<0.01. At 6 months n for cartilage: CS = 32, placebo = 28, for BML: CS = 32, placebo = 29. At 12 months n for cartilage: CS = 30, placebo = 22, for BML: CS = 30, placebo = 23. BL, baseline; m, months.
Cartilage volume loss (%) versus baseline
BML score
The BML data (table 3) showed no differences between the two groups at 6 months. However, at 12 months a trend favouring the CS group was found for the global knee (p=0.062), with a significant difference for the lateral compartment (p=0.035) and the lateral condyle (p=0.044). No difference was found in the trochlea.
Changes in bone marrow lesion scores (BML) versus baseline
Synovitis
No difference was found between the two groups during the double-blind phase for the changes in the mean global synovial thickness (both were −0.1 mm) and in the percentage of subjects having joint swelling (CS, 20%; placebo, 23.5%; p=0.767). Interestingly, patients on concomitant CS and NSAID treatment (n=8) (1.3±0.3 mm) at 6 months demonstrated significantly (p=0.029) less synovial membrane thickness than the placebo group receiving NSAIDs (n=10) (1.6±0.3 mm) and a lower incidence of joint swelling (CS, 0%; placebo, 11.4%; p=0.092).
Symptoms and function
No significant difference in disease symptoms assessed by VAS and WOMAC questionnaires (WOMAC total, pain, stiffness and function) or quality of life (SF-36) at any time point of the study was observed (change in VAS for CS and placebo, respectively, from baseline to 6 months: −14.8±23.7 mm, −20.3±22.1 mm, p=0.359; from baseline to 12 months: −21.0±27.1 mm, −24.7±25.0 mm, p=0.607. Change in WOMAC pain subscale, respectively, from baseline to 6 months: −79.7±105.6, −94.4±96.9, p=0.572; from baseline to 12 months: −99.2±96.7, −124.4±85.3, p=0.327; further data not shown). Paracetamol (rescue medication) was used by 79% of the patients (double-blind n=69, CS n=27, placebo n=28, p=0.766). In the open-label phase (month 6 to 12) NSAID rescue was allowed and used by 76% (open-label n=58, CS n=25, placebo n=19, p=0.761).
Safety
Non-serious adverse events were equally distributed within the two treatment groups except for infections and skin disorders, which were more frequent in the CS group (table 4). None of them were ascribed beyond any doubt to the treatment, nor were the serious adverse events (SAE) related to the medication.
Adverse events
Discussion
The present pilot study provides, for the first time, evidence of the structure protective effect of CS in knee OA patients as early as 6 months into treatment. In addition, the pronounced reduction in cartilage loss found in the lateral tibiofemoral compartment was also associated with a reduction in the size of BML. This finding is interesting as BML are believed to be associated with the progression of cartilage lesions.46,–,51
This study is the first to use quantitative MRI to assess the DMOAD potential of CS in knee OA patients, bringing important information to a field in which the results have been contradictory in the past. The positive results are in line with a number of studies using x-ray technology5,–,8 and with a recent meta-analysis that reported CS to be effective in reducing JSN.52 However, another recent meta-analysis including x-ray trials of glucosamine and CS,53 as well as a structural analysis of the Glucosamine/chondroitin Arthritis Intervention Trial (GAIT)54 in which a non-fluoroscopically guided x-ray technique was used and sample sizes were small, came to the conclusion that there is no treatment effect of CS. In general, the effect size was reported to be small to moderate, demonstrating the need for further trials that may confirm the positive findings of the present trial and shed light on this controversial field.
In the present study, the shorter time (6 months) needed to obtain significant difference demonstrated the superiority of MRI in such studies. MRI has been shown to reliably and quantitatively assess cartilage volume and its changes over time in knee OA in longitudinal15 23 and clinical14 studies. With regard to this study, as age was significantly different in the two groups the results were adjusted where appropriate and no relevant change overall was found. Of note, the observed rate of cartilage loss found in this study lies within the upper range of previous reports.14 43 55 56 Here, CS treatment was found to significantly reduce the cartilage volume loss at 6 months in the global knee, mainly in the lateral tibiofemoral compartment and tibial plateaus. These findings are in accordance with those of a previous MRI multicentre trial14 in which a protective effect with the DMOAD licofelone was also detected as early as 6 months into the study, and was found predominantly in the lateral compartment. Data from x-ray studies showed a protective effect of CS mainly in the medial compartment. These findings are probably related to the design of these studies, as in those trials the JSW was measured only in the medial compartment.5 6 8 A number of hypotheses could explain the predominant positive effect of CS treatment in the lateral compartment, including: (1) lesions are generally less severe in the lateral compartment than in the medial compartment and may be more responsive to treatment; (2) the effect of CS on the medial compartment could also take place at a later time during the treatment schedule (eg, 2 years).7 8 The non-significant effect of the drug seen on the trochlea could reflect the distinct biomechanical environment of the femoropatellar compartment. Our system did not allow for the detection of the cartilage in the patella, which could be considered a limitation of the findings. The significant reduction in cartilage volume loss in the CS group was found to persist until the end of the open phase at the 12-month follow-up. The reduction in the difference of the rate of cartilage loss between the two groups in the double-blind phase (figure 2) could probably be explained by the fact that the placebo group started CS treatment at 6 months. Treatment with CS was effective at reducing both BML and cartilage volume loss in the same anatomical regions; however, a decrease in BML occurred only in the open phase (at 12 months). This finding could suggest that BML are consequential to cartilage degradation and thus reducing cartilage lesions could lead to fewer BML. Alternatively, BML were shown to be involved in an inflammatory/catabolic process57 on which CS could act directly, leading to structural repair. The latter hypothesis is supported by in vitro data showing that CS increases the ratio of osteoprotegerin/receptor activator of nuclear factor-κB ligand, suggesting a positive effect on OA subchondral bone structural changes.31 Data also showed that CS treatment alone did not reduce the synovial membrane thickness (primary endpoint). This finding contrasts with those from animal models26 58,–,61 and the GAIT,62 in which CS treatment was associated with a significant decrease in the incidence of joint swelling, effusion, or both upon clinical examination. The relatively small number of patients in the present pilot study could have been the limiting factor explaining the data.
The effect of the combination of CS with NSAIDs on the synovial membrane thickness and the incidence of joint swelling is interesting with practical clinical impact, and definitely needs future exploration. The absence of differences in disease symptoms between the placebo and CS groups could be explained by the use of rescue medication (paracetamol) as well as NSAIDs, which are strong confounding factors, and this may have masked an underlying symptom-relieving effect of CS. Moreover, as the severity of femoropatellar OA was not assessed, this might have been an additional confounding factor. The impact of the structure-modifying effect of CS on disease symptoms may also become clinically significant only after an extended period of treatment. That question can only be answered by a long-term study. The study design included a double-blind phase (6 months) followed by an open-label phase (6 months) with CS treatment in both groups. This design does not allow for any conclusion regarding the symptom-relieving effects of CS, especially in the open-label phase, as the dropouts after unblinding occurred only in the placebo group resulting in a possible selection bias. The second phase was primarily chosen to gather additional information on the effects of CS on structural change.
The use of multiple analyses to compare the different structural changes has limitations, including the risks of finding significant results only by chance. Because of a relatively small study sample size, imbalances in baseline characteristics between the treatment groups may have had an impact on our results. For instance, even if there is a numerical difference (without statistical significance) between treatment groups for variables such as BML scores and the presence of knee swelling and effusion, adding these additional variables in the ANCOVA model would not yield any additional significant information. Therefore, a confirmation of these results in a larger trial is mandatory.
The safety profile of CS was excellent and confirms the findings of previous reports.5,–,8 62 63 No SAE were found to be related to CS.
In summary, this pilot study demonstrates with the use of quantitative MRI a significant reduction in cartilage volume loss as early as 6 months into treatment with CS and, for the first time, a significant reduction in BML size. These data underline not only the importance of the crosstalk between cartilage and subchondral bone in OA, but also their potential role in the disease process and response to DMOAD treatment. The anti-inflammatory effect of the combination of CS with NSAIDs is a new and interesting finding that deserves confirmation in a definitive study. In conclusion, CS has been shown to be a safe drug with a positive global effect on OA joint structural changes.
Acknowledgments
The authors thank Josée Thériault and André Pelletier for the MRI knee segmentation and Virginia Wallis for her assistance with the manuscript preparation. Lukas Wildi received a grant from the Swiss National Science Foundation and the Fondation du Centre hospitalier de l'Université de Montréal (CHUM).
References
Footnotes
-
Funding This investigator-initiated study was supported in part by a grant from Bioiberica (Barcelona, Spain). Bioiberica was involved only in the design of the study and the approval of the final manuscript.
-
Competing interests J-PR is a consultant for ArthroVision Inc. JM-P and J-PP are consultants for and shareholders in ArthroLab Inc. and ArthroVision Inc. AB, LB and FM received honoraria from ArthroLab Inc. FA is an employee of ArthroVision Inc. MD is a consultant for ArthroVision Inc.
-
Ethics approval This study was approved by the local ethics committees.