Article Text

Abstract
Background: Most registration trials in rheumatoid arthritis (RA) include a placebo arm in the setting of an incomplete response to disease-modifying antirheumatic treatment (DMARD-IR). A minimum duration of 6 months is required despite serious methodological and ethical shortcomings.
Objective: To study whether a 3-month placebo period is sufficient to prove efficacy.
Methods: Meta-analysis of placebo- or active control trials of biological agents in DMARD-IR RA, comparing the contrast in ACR response between experimental and control groups at 3 and 6 months.
Results: Twenty trials yielded 15 placebo and 18 active control contrasts (>10 000 patients). At 3 months active treatment showed a highly significant contrast with placebo for ACR20 and ACR50 in every instance. As all groups improved further the mean contrast at 6 months was unchanged. For ACR70 the contrast was clearly greater at 6 months owing to further improvement only in the experimental groups. In active control trials contrasts were smaller, and for ACR50 and ACR70 these decreased somewhat owing to “catch-up” responses in the control groups.
Conclusion: The placebo phase of registration trials for RA can be limited to 3 months. An accompanying viewpoint proposes that patients receiving placebo should then be switched to standard of care, allowing a more valid and comprehensive assessment, including safety.
Statistics from Altmetric.com
Randomised placebo-controlled trials are required for most new drug applications. In rheumatoid arthritis (RA), placebo is added to background antirheumatic disease-modifying treatment continued in the setting of an incomplete response (DMARD-IR). A minimum of 6 months’ duration has been required by regulatory agencies, although some trials have continued for a year or longer.
In a previous article I have outlined the many disadvantages of this design.1 These include both ethical considerations and problems that jeopardise validity such as the definition of inadequate response, and selective dropout in the placebo group.
To see whether the placebo phase can be shortened this study compared the response rates at 3 and 6 months in a large dataset of trials of biological agents.
Methods
In the context of an indirect comparison meta-analysis between tocilizumab and other biological agents1a the literature was searched for trials of currently licensed and commonly used biological agents in patients with moderate to severe RA who had an incomplete response to DMARDs. To be eligible for the current review, trial treatment had to be constant over 6 months and data on ACR20, ACR50, ACR70 response at both 3 and 6 months had to be available. Where necessary, response rates at 3 months were extracted from figures in the published report. Tocilizumab data was available from Roche clinical reports. Of these, three trials have now been fully published,2 3 4 one is available online,5 and one is only available in abstract form.6 Details of the search and data extraction strategy are available online (Appendix 1).
Trial contrasts were categorised as active control or placebo control, depending on whether or not the control group received treatment expected to work (on top of any background DMARD treatment). Several trials studied more than two groups: mostly placebo and different doses of the experimental drug. In these cases the contrast between placebo and the highest dose (or combination) was included in the placebo control part of the analysis, and the contrast between the active arms in the active control part. Thus the most active treatment arm was used twice. In one active control trial7 the least active treatment arm (methotrexate only) was used twice in the active control part of the analysis: once in the contrast with etanercept, and once in the contrast with etanercept plus methotrexate. No statistical adjustments were made for repeated comparisons.
The ratio of each ACR (20, 50, 70) response rate between control and experimental groups was summarised separately for the placebo and active control contrasts, by weighted Mantel–Haenzsel random effect risk ratios (RevMan v 5 for Mac, Cochrane collaboration: http://www.cochrane.org). This risk ratio expresses the “risk” of response in the experimental group given the response in the control group.
Risk ratios of responses at 3 and 6 months were then compared in a stratified analysis, applying the same weights as in the first step. Finally, for the placebo trials sample size calculations were performed for a range of plausible response rates in the experimental groups.
Results
The search identified 714 potentially relevant studies. Of these, 650 studies did not meet inclusion criteria. Five tocilizumab studies were added yielding a total of 69 studies potentially eligible for this review. Forty-nine had to be excluded after full-text review, yielding a final study set of 20 trials: 16 placebo and four active control trials on 10 514 patients.2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 Full results of the study selection are available online. From the 20 included trials, 15 placebo and 18 active contrasts were extracted: in one three-arm trial, the placebo responses at 3 months were not available from the publication.15 Most patients included in the trials had severe, active and longstanding RA (table 1; more details in online supplementary table 1).
Characteristics of included studies (more details in online supplementary table 1)
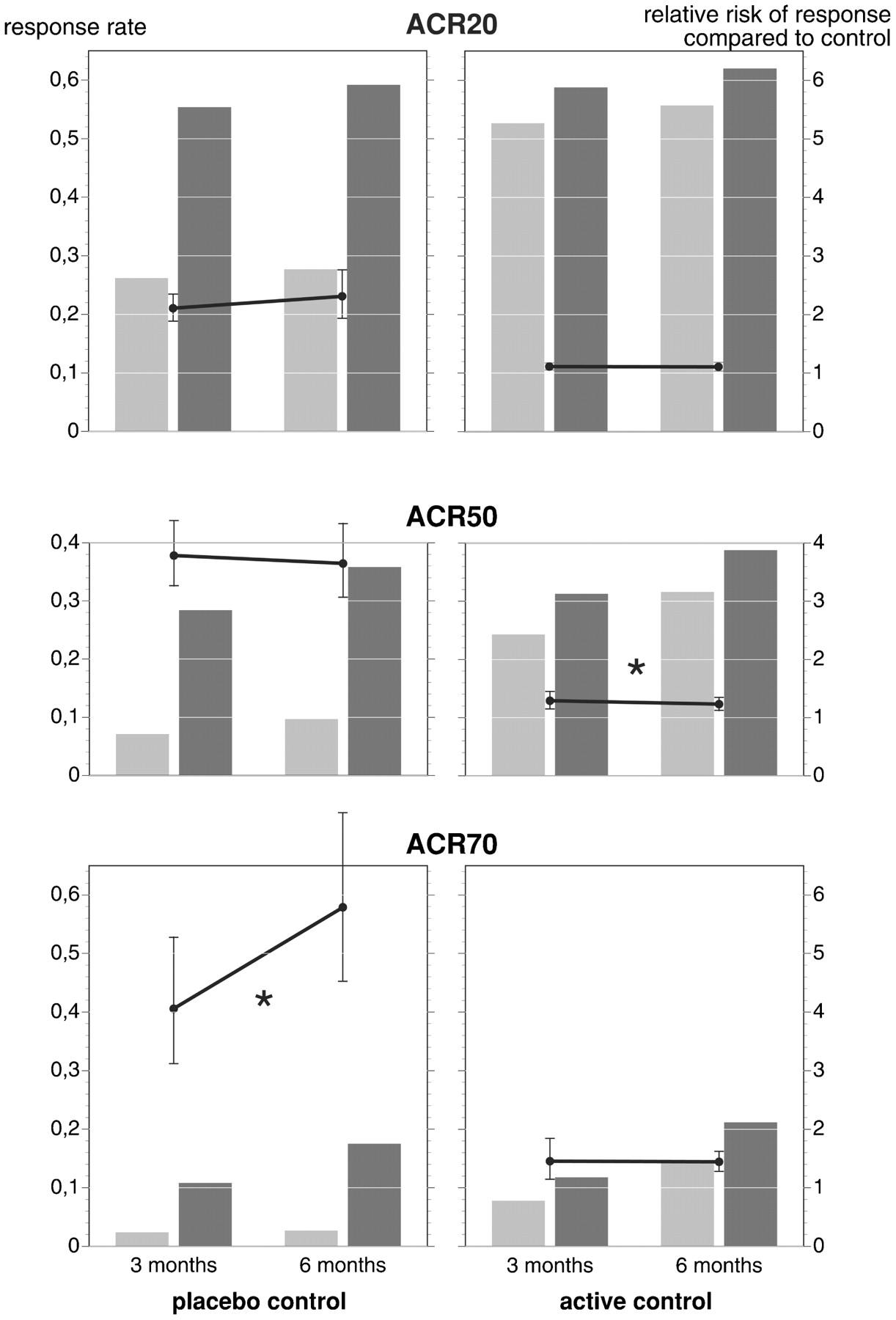
In general, responses were higher at 6 than at 3 months, but this was true for both control and experimental groups (table 2, fig 1). In placebo trials at both 3 and 6 months the contrasts (ie, differences between placebo and experimental groups) were all highly significant for ACR20 and ACR50 levels. For these response cut-off points the mean contrast did not change significantly between 3 and 6 months, marginally increasing for ACR20 and respectively decreasing for ACR50 (fig 1, table 2). Heterogeneity in these comparisons was evident from the range in the ratio of contrasts in individual trials: from 0.4 (3 months better) to 1.9 (6 months better).

{kind=link}
Matrix plot describing ACR20, ACR50 and ACR70 responses (left y axis) at 3 and 6 months, for placebo and active controlled trials. Light bars, control group; dark bars, experimental group. The mean risk ratio with 95% confidence intervals and its change between 3 and 6 months is shown as connected dots (right y axis).
Pooled response rates; contrasts between treatment groups for placebo and active control trials expressed as risk ratios at 3 and 6 months; and the contrast (ratio of risk ratios) between 6 and 3 months.
For ACR70 the contrasts in response were clearly higher at 6 months: at 3 months the contrast between placebo and experimental groups was not significant in four out of 15 trials, decreasing to one out of 15 at 6 months. The “risk” of an ACR70 response on experimental compared with placebo treatment increased from 4.1 at 3 months to 5.8 at 6 months, a 40% increase (p = 0.02; table 2). This was mainly due to an increase of patients meeting ACR70 only in the experimental groups. Finally, in the subgroup of (only two) trials in patients with an incomplete response to tumour necrosis factor contrasts were generally higher, with numerically higher responses at 6 than at 3 months. The small number of trials for each individual drug or drug class precluded meaningful comparisons between them.
As expected, responses in active control groups were much higher than those seen in placebo, resulting in a correspondingly smaller contrast with the experimental groups. For ACR20 the contrasts did not change significantly between 3 and 6 months. For ACR50 and ACR70 the contrast actually decreased somewhat (significant for ACR50), mostly because the response rate in the control groups increased more than that in the experimental groups—that is, a “catch-up” response.
Calculations for the placebo setting suggested sample sizes for both ACR20 and ACR50 are well below 100 patients per group for a range of plausible response rates (supplementary data in online Appendix 2 and supplementary figure to Appendix 2).
Discussion
This study demonstrates that for currently available biological agents, a 3-month placebo phase is sufficient to demonstrate efficacy in signs and symptoms of RA.
Although a broad range of large key trials was included, many more could not be considered simply because the trial report was incomplete. As recently recommended by EULAR, all trial reports should include the results of the RA core set as well as ACR and EULAR response criteria at key time points.22 Editors can easily facilitate this by allowing publication of web-only material. However, the principal finding need not be demonstrated in all published trials to be valid. Even the current selection included trials that “benefited” from a longer placebo phase. Irrelevant benefit, I would argue as in all trials the difference at 3 months between active and placebo was highly significant for both ACR20 and ACR50 anyway, and in most this also applied to ACR70. Trials with 100 patients/group have over 90% power to show such differences in ACR20 and ACR50.
The requirement for 6 months’ stable treatment suggests that the results are not directly applicable to some “tight control” strategies of treatment that require switching or modifying treatment when an adequate response is not seen within 3 months. However, these trials are going to be restricted to using 3-month responses exclusively anyway. The study results do suggest that most current (rapidly acting) agents still need 6 months to develop their full effect. So registration trials should run for at least 6 months, but only 3 months of these need to be a comparison against placebo. As explained in the accompanying viewpoint in this issue, this opens the way to novel trial designs in which placebo patients are mandatorily switched to standard treatment after 3 months, or re-randomised to standard versus experimental treatment (see article on page 4).23 Such designs create new complexities but also produce data comparing the new drug with standard active treatment early in the development phase. Imagine such data being available to the clinician at the time of registration of the new drug! For active control studies, although much information can be gathered in first 3 months, there is little or no justification for a 3-month study period in the context of a chronic disease usually requiring lifelong treatment.
There are concerns that go beyond the demonstration of short-term efficacy. Authorities and doctors are also interested in the full extent and the durability of effect, as well as safety. While not dealt with by the current study, a recommendation to limit the placebo phase to 3 months need not affect the data collection necessary to study these issues. Once separation from placebo is demonstrated, both full effect and durability can even be documented by a within-group comparison (change from baseline) in the experimental group continuing to receive treatment. For safety, the current practice of comparison with a depleted placebo group is probably less valid than a comparison with a group that received proper treatment after 3 months of placebo.
For structural damage, current guidelines require trials of 1 or 2 years before a label can be given for a protective effect. In this context all the disadvantages of long placebo periods apply with respect to the validity of the comparisons being made. Data are available suggesting that a difference in damage progression can be demonstrated at 3 months in reasonable sample sizes (about 100 patients per group).24 Again, both full effect and durability of effect can then be demonstrated by within-group comparisons and comparisons with a placebo group that switches to proper treatment after 3 months.
In conclusion, a 3-month placebo phase is sufficient to demonstrate efficacy in the treatment of signs and symptoms of RA. I propose that placebo patients should then be switched to standard of care, allowing a more valid and comprehensive assessment including safety.23
Acknowledgments
I am grateful to Neil Wintfeld of Roche Laboratories, Nutley, USA for helpful comments; Adrian Kielhorn, F Hoffmann-La Roche, Basel, Switzerland for help in collecting the data; and F Hoffmann-La Roche, Basel, Switzerland for allowing use of their dataset.
REFERENCES
Supplementary materials
Web Only Data 69/1/186
Files in this Data Supplement:
Footnotes
▸ Additional data are published online only at http://ard.bmj.com/content/vol69/issue1
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.