Article Text

Abstract
Objective: To evaluate the long-term effectiveness and tolerability of adalimumab in the treatment of psoriatic arthritis (PsA).
Methods: Patients with PsA who completed a 24-week, double-blind study of adalimumab versus placebo were eligible to enroll in an open-label extension study and receive adalimumab 40 mg subcutaneously every other week for up to an additional 120 weeks. At the time of this analysis, available efficacy evaluations throughout 2 years of treatment (n = 245) included American College of Rheumatology (ACR) 20%, 50% and 70% improvement scores, measures of joint disease and skin disease, disability and quality of life; modified total Sharp scores (mTSS) were available for 2.75 years of treatment for patients who received adalimumab in the 24-week study.
Results: After 24 weeks of double-blind treatment, the mean change in mTSS was −0.2 for the adalimumab group (N = 144) and 1.0 for the placebo group (N = 152; p<0.001), and outcomes for all individual ACR component variables were significantly improved in adalimumab compared with placebo-treated patients. Compared with 24-week responses, inhibition of radiographic progression and improvements in joint disease were maintained in most patients during long-term, open-label adalimumab treatment. Also, improvements in skin disease were maintained, with >20% of patients achieving the strict criterion of psoriasis area and severity index 100. The nature and frequency of adverse events during long-term adalimumab treatment were consistent with the safety profile during short-term treatment.
Conclusions: The clinical and radiographic efficacy of adalimumab demonstrated during short-term treatment was sustained during long-term treatment. Adalimumab has a favourable risk–benefit profile in patients with PsA.
Trial registration number: NCT00195689.
Statistics from Altmetric.com
Psoriatic arthritis (PsA) is an inflammatory arthritis that occurs in up to one-third of patients with psoriasis and is usually diagnosed years after the skin disease appears.1 2 More than 50% of patients with PsA experience progressive, erosive arthritis that is often accompanied by functional impairment.3–6 Patients with psoriasis and PsA suffer functional impairments that are associated with direct healthcare costs (nearly US$650 million/year), impaired health-related quality of life and substantial work-related disability, including a lower rate of employment.1 2 7–10
Treatment for moderate to severe PsA traditionally has included the same disease-modifying antirheumatic drugs (DMARD) used for rheumatoid arthritis (RA) (eg, methotrexate, leflunomide, azathioprine, gold and sulfasalazine), despite there being relatively little evidence for the efficacy of these drugs in PsA and essentially no evidence that they slow joint destruction in PsA.11–16 In fact, the number of joints affected and the extent of joint damage frequently increase in patients with PsA despite treatment with salicylates, DMARD or glucocorticoids.5 17–20
Adalimumab is a fully human, anti-tumour necrosis factor (TNF) monoclonal antibody that has been shown to have efficacy, alone or in combination with methotrexate, in the treatment of moderate to severe RA.21–23 The Adalimumab Effectiveness in Psoriatic Arthritis Trial (ADEPT) demonstrated that, in patients with PsA, adalimumab significantly improved skin and joint manifestations, lessened disability caused by joint damage, inhibited structural changes on radiographs and improved health-related quality of life (HRQOL) while being generally well tolerated during 24 weeks of therapy.24 25 Patients who completed the 24-week ADEPT study were eligible to enroll in a 120-week open-label extension to evaluate the long-term efficacy and safety of adalimumab. The 48-week results of the open-label extension demonstrated that adalimumab improved joint and skin manifestations, reduced disability and inhibited radiographic progression during long-term treatment of patients with PsA.25 Here we report the clinical efficacy and safety of adalimumab for 2 years of treatment and the radiographic efficacy for 2.75 years of treatment.
METHODS
Patients and protocol
Patients who completed the original 24-week double-blind ADEPT study (N = 289) were eligible for this open-label extension study and 285 patients elected to enroll. Patients continued to receive adalimumab 40 mg subcutaneously every other week for up to 144 weeks of total adalimumab exposure. The first adalimumab exposure occurred at the start of the double-blind lead-in study for patients randomly assigned to receive adalimumab in ADEPT and at the start of the open-label extension study for patients randomly assigned to receive placebo in ADEPT. Patients who received placebo during the lead-in study thus had a duration of adalimumab exposure that was 24 weeks less than patients who received adalimumab during the lead-in study. After 12 weeks in the extension study, patients who did not have a 20% or greater improvement compared with baseline in the tender joint count and the swollen joint count were allowed to increase the adalimumab dosage to 40 mg a week. Non-steroidal anti-inflammatory drugs (NSAID), prednisone, and/or DMARD could not be initiated during the extension study but were continued for patients who were receiving these medications at the start of the extension study; tapering of any concomitant medications for the treatment of PsA was allowed after 6 weeks of treatment.
Descriptions of the clinical efficacy, radiographic efficacy and safety assessments during the open-label extension study were published previously,25 as were HRQOL measures.26
Statistical analyses
For all analyses, the efficacy and safety populations comprise all patients (N = 298) who received any dosage of adalimumab in the double-blind portion of ADEPT or in the open-label extension study. Clinical efficacy and safety measures at all time points were analysed and are reported based on the duration of adalimumab exposure, with the exception of radiographic data, which was analysed and is reported from the baseline of ADEPT. For radiographic data, results were analysed and are reported for 144 weeks (∼2.75 years) of adalimumab exposure. For patients without a week 144 modified total Sharp score (mTSS), the week 96 mTSS was used to impute the week 144 score. For all other data (eg, clinical assessments of joint and skin disease, HRQOL assessments), results are reported for 104 weeks (2 years) of adalimumab exposure based on available data at the time of this analysis. Only patients with at least 3% body surface area involvement at enrollment in ADEPT were included in the analyses of psoriasis area and severity index (PASI) and dermatology life quality index (DLQI). All data are last observation carried forward (LOCF) unless otherwise noted. For patients whose adalimumab dosage was increased from 40 mg every other week to 40 mg a week, the last observation before dosage increase was carried forward when analysing American College of Rheumatology (ACR) 20%, 50% and 70% improvement score responses; PASI 50, PASI 75, PASI 90 and PASI 100 responses; psoriatic arthritis response criteria (PsARC) and the physician’s global assessment of psoriasis.
RESULTS
Study population
The baseline characteristics of patients who continued adalimumab treatment in the open-label extension study were similar to those of the 313 patients who enrolled in ADEPT.24 In ADEPT, the overall population of treated patients (151 in the adalimumab group and 162 in the placebo group) had mean (SD) baseline scores of 25 (SD 18) for tender joint count, 14 (SD 12) for swollen joint count, 1.0 (SD 6) for health assessment questionnaire disability index (HAQ DI) and 20.8 (SD 40.9) for mTSS. These values are consistent with long-standing moderate to severe PsA.24 During the open-label extension period, 44 patients discontinued adalimumab treatment. The primary reasons for discontinuation were adverse event (n = 10), unsatisfactory therapeutic effect (n = 12), withdrawal of consent (n = 8), death (n = 3), loss to follow-up (n = 1) and other (n = 10).
Adalimumab exposure
The mean duration of treatment for the 298 patients who received at least one dose of adalimumab was 699 days (approximately 100 weeks) (median 785 days; range 26–785). The adalimumab dosage was increased to 40 mg every week for 54 (18.9%) patients. The mean duration of adalimumab treatment for these 54 patients was 542 days (approximately 77 weeks) (median 640 days; range 21–777). At week 12, the first time point in the open-label extension study when a dosage increase was allowed, 38 patients changed to a dosage regimen of adalimumab 40 mg a week; the adalimumab dosage was increased for the remaining 16 patients at one of the regularly scheduled clinic visits that occurred at 12-week intervals between week 24 and week 76 or at week 92.
Radiographic efficacy
The 24-week, double-blind portion of ADEPT demonstrated that, compared with placebo, adalimumab significantly inhibited structural deterioration of joints as seen on radiographs. The mean change in mTSS was −0.2 for the adalimumab group (N = 144) and 1.0 for the placebo group (N = 152; p<0.001).24 At week 24, 91.0% of adalimumab-treated patients had no radiographic progression (mTSS change ⩽0.5) compared with 71.1% of placebo-treated patients.24 At 48 weeks (24 weeks into the open-label extension study), adalimumab continued to inhibit structural damage in those patients who had received adalimumab during the first 24 weeks of ADEPT (mTSS mean change −0.1 at week 24 and 0.1 at week 48, n = 133).25 The mean changes in mTSS for patients who received placebo for 24 weeks followed by adalimumab for 24 weeks (N = 141) were 0.9 at week 24 and 1.0 at week 48.25
Table 1 demonstrates the percentage of patients with a decrease (<−0.5 units) or no change (<−0.5 to 0.5 units of change) or an increase (>0.5 units of change) in the mTSS over different study periods, from baseline of ADEPT to week 144. This analysis set included all patients who had a week-48 and a week-96 or week-144 radiographic assessment (placebo/adalimumab, N = 128; adalimumab, N = 115). To week 24, 70.3% (90/128) of patients receiving placebo demonstrated no progression compared with 89.6% (103/115) of adalimumab-treated patients. Of the 115 adalimumab-treated patients, 88.7% (n = 102) had a decrease/no change in mTSS to week 48 and 79.1% (n = 91) had a decrease/no change in mTSS to week 144. After week 24 of ADEPT, all patients originally randomly assigned to receive placebo were switched to open-label adalimumab treatment. The percentage of placebo/adalimumab patients (N = 128) with no progression from weeks 24 to 144 was 77.3% (99/128); this percentage was similar to the 79.1% (91/115) of patients originally randomly assigned to receive adalimumab who had a decrease/no change in mTSS from baseline to week 144. These results demonstrate the benefit of adalimumab treatment in inhibiting structural joint damage.
To demonstrate further the maintenance of radiographic inhibition, patients who were originally randomly assigned to receive adalimumab in ADEPT who had no progression from baseline to week 48 were evaluated at week 144 to determine the percentage of patients with sustained inhibition of radiographic progression as defined by a decrease/no change in the mTSS. Of the 102 patients who had no progression from baseline to week 48, 86 (84.3%) continued to demonstrate no radiographic progression at week 144. The effectiveness of adalimumab in inhibiting radiographic joint deterioration was thus maintained for a large majority of patients throughout 144 weeks of adalimumab treatment.
For the same radiographic analysis set (adalimumab/placebo, N = 128; adalimumab, N = 115), mean changes in mTSS are shown in table 2. From baseline to week 24 of ADEPT, the mean change in mTSS was −0.1 (SD 1.2) in adalimumab-treated patients (N = 115) compared with 0.8 (SD 2.42) in placebo-treated patients (N = 128). Once patients initially treated with placebo began receiving adalimumab, the mean changes in mTSS were similar in the placebo/adalimumab and adalimumab treatment groups (0.0 (SD 3.03) and 0.2 (SD 1.43), respectively) from weeks 24 to 48.
From week 48 to week 144, the mean changes in mTSS for the placebo/adalimumab (N = 128) and adalimumab (N = 115) groups were 0.1 (SD 5.24) and 0.4 (SD 2.61), respectively. These differences in mean changes in mTSS from week 48 to week 144 in the two treatment groups suggest that patients treated continuously with adalimumab had less progression of joint damage compared with patients who switched from placebo to adalimumab treatment after week 24. To explore this unexpected finding further, additional analyses were completed to investigate the mean changes in mTSS over time for patients with and without radiographic progression from baseline to week 24 of ADEPT.
Subgroup analysis of patients with and without radiographic progression to week 24 of ADEPT
Among adalimumab-treated patients with no progression from baseline to week 24 (non-progressors, table 2), inhibition was sustained during adalimumab therapy to week 144 (mean change in mTSS from week 24 to 144 = 0.2). For patients who initially received adalimumab and had progression from baseline to week 24, the mean change in mTSS continued to increase from weeks 24 to 144. By contrast, for patients who initially received placebo and had progression from baseline to week 24, progression was stabilised by adalimumab treatment, with a mean change in mTSS of −0.1 from week 24 to week 144. For the greater progression exhibited in the adalimumab-treated progressor group (table 2), it is important to note that the number of patients in this subgroup was small (n = 12), and these patients had much more aggressive, erosive disease at baseline (mean mTSS 74.9 (SD 96.4)) compared with the adalimumab-treated non-progressor group (16.1 (SD 31.9); p<0.001). There were no statistically significant differences in any other baseline demographic or clinical characteristics between the adalimumab-treated progressors and non-progressors. Overall, this subanalysis demonstrates that the mean changes in mTSS in the adalimumab group from week 48 to week 144 were driven by those patients who had radiographic progression in the first 24 weeks of adalimumab treatment.
Joint space narrowing and joint erosion components of the modified total Sharp score
Between week 48 and week 144, for patients originally randomly assigned to receive adalimumab in ADEPT (N = 115), the mean change in the joint space narrowing component of the mTSS was 0.4 (SD 1.59), and for patients who received placebo and then switched to adalimumab (N = 128) at week 24 of ADEPT, the mean change in the joint space narrowing component was 0.3 (SD 1.96). Over the same period of time, the joint erosion component of the mTSS did not change in the adalimumab group (mean change 0.0 (SD 1.37)) and decreased slightly in patients who switched from placebo to adalimumab (mean change −0.2 (SD 3.85)).
Joint disease
The percentages of patients achieving ACR20, ACR50 and ACR70 in 2 years of adalimumab treatment (N = 298) are illustrated in fig 1. The ACR20 response was achieved by 58.7% (165/281) of patients at week 48 and 57.3% (161/281) of patients at week 104 based on an LOCF analysis. The percentages of patients achieving the stricter response criteria of ACR50 and ACR70 increased over 2 years of adalimumab treatment, from 42.7% (120/281) of patients achieving an ACR50 response at week 48 to 45.2% (127/281) at week 104 and from 27.8% (78/281) of patients achieving an ACR70 response at week 48 to 29.9% (84/281) at week 104. The percentage of patients achieving PsARC was 65.9% (195/296) at week 48 and 63.5% (188/296) at week 104. As reported,24 at baseline in ADEPT, 117 patients had dactylitis and 118 patients had enthesitis. Mean improvements at week 24 in these exploratory endpoints were greater for adalimumab patients, but the changes were not statistically significant.24 The dactylitis mean change from baseline remained constant from 48 weeks of adalimumab exposure (mean change from baseline −1.3 (SD 3.4) units) in 104 weeks of adalimumab treatment (mean change from baseline −1.4 (SD 3.7) units). From week 48 to week 104, the enthesitis mean change from baseline remained constant at −0.4 (SD 1.1) units. These data indicate that joint-related improvements that were present after 48 weeks of adalimumab therapy were maintained throughout 2 years of therapy.

Percentages of patients achieving American College of Rheumatology (ACR) 20%, 50% and 70% improvement score response status to week 104 based on the duration of exposure to adalimumab (including those patients originally randomly assigned to placebo). Data are last observation carried forward. For patients who had an adalimumab dosage increase, the last observation before the dosage increase was carried forward. N = 281 at all time points to week 104. Patients originally randomly assigned to receive placebo had a rapid response when switched to adalimumab at week 24.25
Skin disease
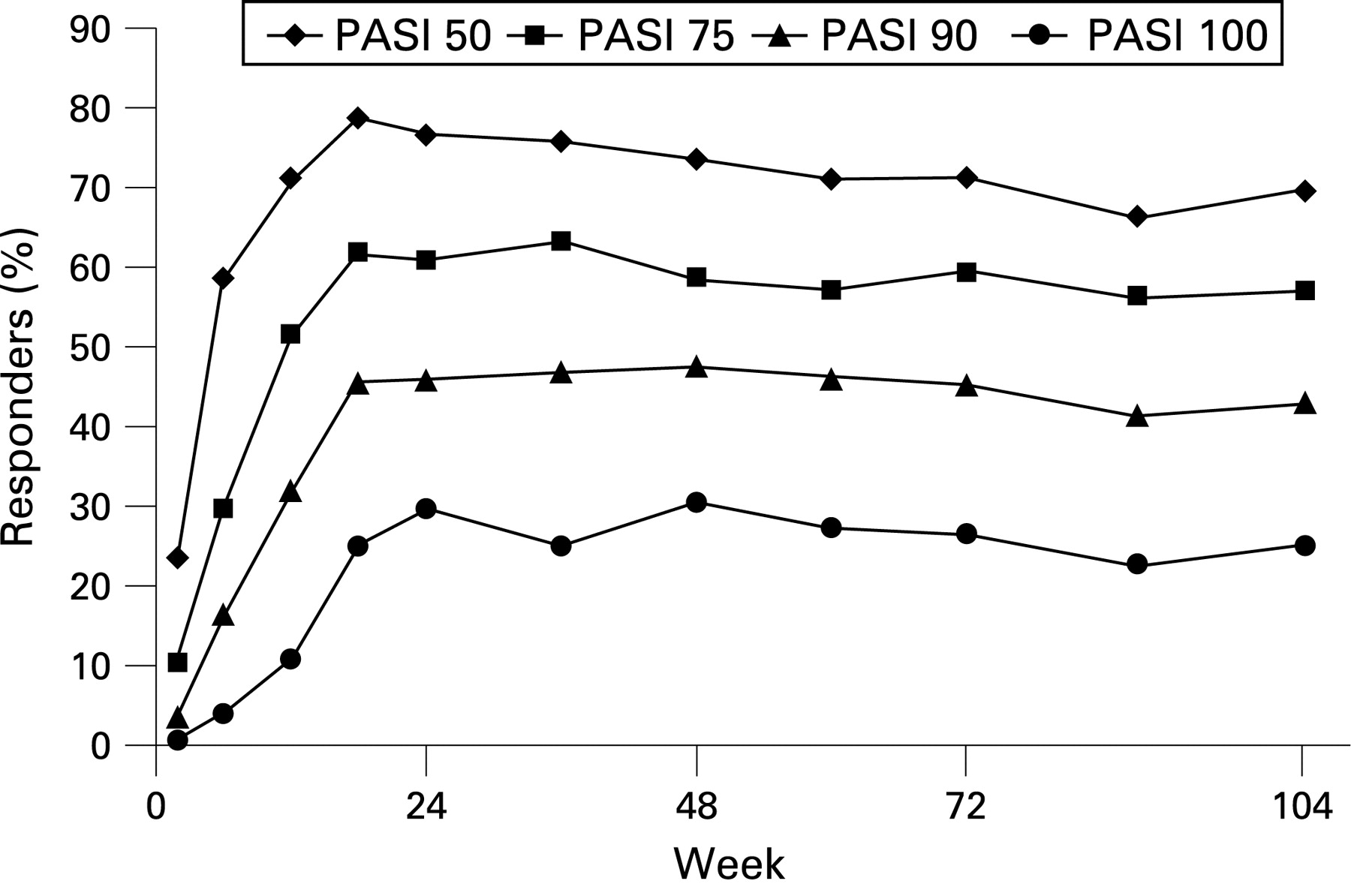
Skin assessments were restricted to patients with at least 3% body surface area involvement (N = 128) at enrollment, as reported previously.24 25 The percentage of patients achieving the PASI 50, PASI 75, PASI 90, or PASI 100 response criteria changed by 10% or less from week 48 in 2 years of adalimumab treatment (fig 2). Notably, the percentage of patients achieving PASI 100 (a particularly high threshold of response for skin disease) remained above 20% between weeks 48 and 104 of adalimumab treatment. The mean percentage improvement in PASI from baseline was sustained within a range of 5 percentage points from week 48 (68.5 (SD 52.0)) to week 104 (63.9 (SD 58.6)). For the physician’s global assessment of psoriasis, the percentages of patients falling into the “clear” or “almost clear” categories were 6.2% (8/129) at baseline, 63.6% (82/129) at week 48 and 56.6% (73/129) at week 104 (LOCF analyses). Thus, skin-related improvements that were present after 48 weeks of adalimumab therapy25 were maintained throughout 2 years of therapy for most patients.
{kind=link}
{kind=link}
Percentages of patients achieving psoriasis area and severity index (PASI) 50, PASI 75, PASI 90 and PASI 100 response status to week 104 based on the duration of exposure to adalimumab (including those patients originally randomly assigned to placebo). PASI was assessed only for patients with at least 3% body surface area involvement at enrollment. Data are last observation carried forward. For patients who had an adalimumab dosage increase, the last observation before the dosage increase was carried forward. N = 128 at all time points to week 104.
Health-related quality of life
Results of the HRQOL assessments at week 24 of the open-label extension have previously been reported26 and are included in table 3 for reference. At week 24 of ADEPT, all HRQOL assessments were statistically significantly improved in adalimumab-treated patients compared with placebo-treated patients, with the exception of the short form 36 health survey (SF-36) mental component summary (MCS) mean score and the SF-36 role–emotional domain mean score.26
The mean change from baseline in the HAQ DI remained −0.3 units from week 48 to week 104, and the observed percentage of patients with HAQ DI of 0 increased from 35.8% at week 48 to 38.5% at week 104 (table 3). The observed percentage of patients achieving the minimum clinically important difference (MCID) in HAQ DI (⩾−0.3 point change from baseline)27 was 48.7% at week 48 and 47.6% at week 104.
Mean scores for the SF-36 physical component summary (PCS) and the MCS scores remained unchanged throughout the study (table 3). The observed percentages of patients who achieved the MCID in the SF-36 (⩾3 points change from baseline)28 increased slightly from weeks 48 to 104 for the PCS (76.4% to 78.6%) and for the MCS (42.5% to 50.0%).
The mean absolute functional assessment of chronic illness therapy–fatigue (FACIT–F) score had increased (improved) by 6.7 (SD 9.8) units from baseline at week 48 and by 6.1 (SD 10.4) units at week 104 (table 3). The observed percentage of patients who achieved the MCID (⩾3 points change from baseline) increased from 66.3% at week 48 to 76.7% at week 104.
The mean absolute change from baseline in the DLQI varied minimally between week 48 (−6.1 (SD 6.9)) and week 104 (−5.8 (SD 7.4); table 3). Based on observed data, the percentage of patients who achieved the MCID (a change of ⩾−5.7 points in the DLQI from baseline) was 49.5% after 48 weeks and 56.3% after 104 weeks of adalimumab treatment. At week 48, 68.5% (76/111) of patients achieved a DLQI score of 0 or 1 and at week 104, 68.8% (11/16) of patients had a score of 0 or 1 (observed data).
Improvements in the patients’ assessment of pain and the patients’ global assessment of disease activity were maintained from week 48 to week 104 (table 3).
Safety
Adalimumab was generally well tolerated throughout 2 years of adalimumab exposure (N = 298). There were no clinically meaningful differences between the first 48 weeks of adalimumab exposure25 and the entire 104 weeks of adalimumab exposure. The most common adverse events in 2 years of exposure were similar to the type of adverse events observed in the 24-week ADEPT study24 and in 48 weeks of adalimumab treatment,25 with upper respiratory tract infection occurring in 21.5% of patients (64/298), nasopharyngitis occurring in 17.4% (52/298) and sinusitis occurring in 10.7% (32/298). Of the 298 patients in the 2-year safety population, 273 (91.6%) experienced at least one adverse event (table 4). Fifty patients (16.8%) experienced at least one serious adverse event. The most common serious adverse event was cholelithiasis, seen in three patients (1.0%). The following serious adverse events were each reported in two patients (0.7%): myocardial infarction, appendicitis, urinary tract infection, osteoarthritis, psoriatic arthropathy, convulsion and nephrolithiasis. Twenty patients (6.7%) discontinued study drug as a result of an adverse event; however, no single type of adverse event was associated with discontinuation in more than one patient. Throughout 2 years of adalimumab exposure, 7.0% (21/298) of patients ever had an alanine aminotransferase value three or more times the upper limit of normal, and 4.7% (13/298) of patients ever had an aspartate aminotransferase value three or more times the upper limit of normal. As previously reported, most changes in transaminase values were transient and resolved during continued adalimumab treatment.24 25
During the first 48 weeks of adalimumab exposure, there were no reports of tuberculosis, demyelination, lymphoma or carcinoma, drug-induced lupus, or congestive heart failure.25 Throughout 2 years of adalimumab exposure, one patient had peritoneal tuberculosis and four patients experienced opportunistic infections (oral candidiasis). One patient had non-Hodgkin’s B-cell lymphoma, two patients had basal cell carcinoma and one patient had neuroendocrine carcinoma of the skin. There were no reports of central nervous system demyelinating disease, lupus-like syndrome, congestive heart failure, or adalimumab-related allergic reactions.
Three deaths occurred among the 298 patients. One patient experienced cardiopulmonary arrest and myocardial infarction that were probably not related to study drug. Another patient experienced sudden death that was attributed to acute pulmonary oedema and was considered possibly related to study drug. The third death was caused by myocardial infarction 104 days after the last dose of adalimumab and was probably not related to study drug.
DISCUSSION
ADEPT is the largest randomised controlled study to date that investigated the use of a TNF antagonist for the treatment of patients with PsA. The ADEPT 24-week results established that adalimumab was more efficacious than placebo in treating arthritis and skin disease and inhibiting radiographic progression in PsA, and significantly improved physical function and HRQOL while being well tolerated.24 26 Patients completing ADEPT could enroll in an open-label extension trial, during which they received 40 mg adalimumab subcutaneously every other week for up to a total of 144 weeks. Interim results from the open-label extension study demonstrated that clinical efficacy, inhibition of radiographic progression and a favourable risk–benefit profile of adalimumab were maintained throughout 48 weeks of treatment.25 The analyses reported here establish the clinical efficacy of adalimumab for at least 2 years of treatment and the inhibition of structural progression of PsA for at least 2.75 years of treatment. The favourable risk–benefit profile of adalimumab was also sustained during long-term treatment of patients with PsA and is consistent with that of other TNF antagonists.29 30
The inhibition of joint damage previously demonstrated throughout 48 weeks of adalimumab treatment25 was sustained for 144 weeks of treatment. Among patients originally randomly assigned to receive adalimumab in ADEPT who had no radiographic progression of structural disease at week 48, 84.3% continued without progression to week 144. Patients who switched to adalimumab treatment after 24 weeks of placebo demonstrated inhibition of radiographic progression, as measured by a mean mTSS that was comparable in magnitude to the inhibition of radiographic progression measured in patients who were treated continuously with adalimumab. In addition, placebo-treated patients who had radiographic progression to week 24 of ADEPT had inhibition of progression after switching to adalimumab. These results suggest that treatment delays may contribute to the progression of structural damage in patients with PsA.
Further analysis of patients with and without radiographic progression from baseline to week 24 of ADEPT demonstrated that the mean increase in mTSS to week 144 for patients originally randomly assigned to receive adalimumab was attributable to those patients who had radiographically defined progression of structural damage from baseline to weeks 24 and 48. This finding suggests that there may be a small subgroup of patients who do not respond to adalimumab despite continued treatment. Additional analyses (data not shown) indicated that there were no clinical responses to adalimumab treatment that correlated with radiographic progression versus non-progression. The 12 adalimumab-treated patients who had radiographic progression during the first 24 weeks of ADEPT continued in the open-label extension to week 144, suggesting a clinical benefit of adalimumab despite structural disease progression.
In addition to inhibiting radiographic progression in patients with PsA, adalimumab resulted in sustained improvement of joint and skin-related symptoms throughout 2 years of treatment. Improvements in PsARC, dactylitis and enthesitis were maintained between week 48 and week 104. The percentage of patients achieving ACR20 was sustained and the percentages of patients achieving ACR50 and ACR70 increased slightly in 2 years of adalimumab treatment. Improvements in PASI that were seen at week 48 were constant to week 104. Approximately one in five patients achieved and sustained PASI 100 during long-term adalimumab treatment, indicating full clearance of skin signs of psoriasis. This magnitude of improvement in skin disease has not been demonstrated with the use of other TNF antagonists during long-term treatment of PsA. Of the various clinical responses, PASI 50 was found to be a sensitive indicator of reduced radiographic progression in patients with PsA treated with adalimumab for 24 weeks.31 Although the trend was still present after 2 years of adalimumab treatment, the correlation between PASI 50 response and reduced radiographic progression was no longer statistically significant. These sustained improvements in joint and skin-related symptoms probably contributed to HRQOL improvements that were maintained throughout 2 years of adalimumab treatment. DLQI scores of 0 to 1 indicate that skin disease has no effect on a patient’s quality of life,32 and DLQI scores of 0 or 1 were achieved by approximately 60% of patients during long-term adalimumab treatment.
The safety profile of adalimumab during long-term treatment of PsA was consistent with the safety profile during short-term treatment. There were no clinically meaningful changes in the type and frequency of adverse events compared with 24 or 48 weeks of adalimumab treatment.24 25 With the exception of a marked decrease in mean C-reactive protein concentrations (a known marker for clinical improvement), changes in laboratory values from weeks 48 to 104 were not clinically significant. There was no indication of an increase in TNF-associated adverse events, including serious infections such as tuberculosis, or in malignancies, demyelination, congestive heart failure and lupus-like syndrome.
The safety profile of adalimumab demonstrated throughout 2 years of exposure in patients with PsA was consistent with that reported for more than 10 000 patients in RA clinical trials21–23 33 and also with the safety profile of the adalimumab postmarketing safety database.33
The short-term clinical benefits of adalimumab therapy in patients with PsA are maintained over 2 years of treatment and the ability of adalimumab to inhibit structural progression of the disease is maintained over 2.75 years of treatment. Compared with short-term adalimumab treatment, there were no additional safety concerns during long-term treatment. Overall, adalimumab presents a favourable risk–benefit profile in patients with PsA.
Acknowledgments
The authors acknowledge the assistance of Marilyn Collicott and Carol Feige for study logistics, Michele Olds for statistical support and Jennifer Dinelli for data management (all of Abbott Laboratories). In addition, the authors thank Dana L Randall, JK Associates, Inc, for manuscript preparation and Michael A Nissen, of Abbott Laboratories, for manuscript editing assistance. The authors appreciate the continued efforts of all members of the ADEPT Study Group.
REFERENCES
Footnotes
Competing interests: PJM has received research grants and speaker’s bureau honorarium from Abbott Laboratories and has served as a consultant for Abbott Laboratories. DDG has received consulting fees and honoraria from Abbott, Amgen, Centocor, Schering and Wyeth and received unrestricted research and education funds from Abbott, Amgen-Wyeth and Schering. PO has received consulting fees or honoraria from Abbott and Amgen. CTR has received consulting fees and honoraria from Abbott, Centocor, Wyeth and Biogen. FVdB has received speaker’s bureau honorarium and has served as a consultant for Abbott Laboratories. JTS has received consulting fees or honoraria from Abbott and Amgen. GTDT reports no competing interests. JM, RJP and RLW are employees of Abbott Laboratories and own shares of Abbott stock.
Funding: The research reported here and the preparation of this manuscript were funded by Abbott Laboratories.
Contributors: The ADEPT Study Group included experts from academic institutions in Europe and the United States and members of Abbott Laboratories who designed the original clinical trial. Clinical data were collected and analysed by Abbott Laboratories. All authors contributed to manuscript development and reviewed and approved the content of the submitted manuscript.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.