Article Text

Statistics from Altmetric.com
Why the effect of excess body weight is greater at the knee
In their study, Reijman et al1(see page 158) report findings that show an association between an increased body mass index (BMI) and greater risk of both incident knee osteoarthritis and knee osteoarthritis progression, but no association between an increased BMI and risk of either incident or progressive hip osteoarthritis. These results confirm what previous studies—that is, studies that were not specifically designed to look at the effect of BMI on the knee and the hip—had hinted at, that BMI has no effect or a smaller effect at the hip than at the knee. As the first study in which BMI effects on the knee and hip were examined in the same population, the study by Reijman et al is a landmark study.
In the literature, summarised by Reijman et al1 in this issue of the journal, the evidence supporting a BMI effect on risk of incident knee osteoarthritis is strong, particularly in women. For example, in a longitudinal study of the Chingford population (women, mean age 54 years), belonging to the top BMI tertile was associated with an increased risk of knee osteoarthritis (odds ratio (OR) 2.38, 95% confidence interval (CI) 1.29 to 4.39) in adjusted analyses.2 In Framingham participants, higher BMI increased the risk of knee osteoarthritis (OR 1.6/5 unit increase, 95% CI 1.2 to 2.2), as did increase in weight (OR 1.4/10 lb increase in weight).3 Findings were confirmed in women but not men perhaps because of the smaller number of incident cases in men.
By contrast, several studies, as noted by Reijman et al,1 have not detected any influence or only a modest effect of BMI on knee osteoarthritis progression, whereas they did disclose other risk factors for progression. In studies of people with hip osteoarthritis, factors that increased the likelihood of disease progression included age, female sex, hip pain and baseline hip joint space width in the Rotterdam study4; hip pain, femoral osteophytes, superolateral joint space narrowing and subchondral bone changes in the Study of Osteoporotic Fractures5; and female sex, older age at symptom onset and higher Kellgren and Lawrence (K/L) grade at entry in the study by Ledingham et al.6 None of these studies suggested that BMI had any effect on hip osteoarthritis progression.
Each of these previous studies examined the BMI effect, looking either at the hip or at the knee. Looking at the hip and the knee in one study of one population addresses the concern that any difference in BMI effect between the joints could be attributed to racial or ethnic differences between populations studied or to methodological differences between studies, but not to differences between the two joints as such.
The study by Reijman et al has several additional strengths. The sample is population based. The study looks at incidence and progression outcomes in the same study. If the effect on incidence differed from that on progression when these outcomes were examined in separate studies, it would be possible that the difference was linked to methodological differences between studies. Dichotomous outcome definitions are wisely applied, given the use of conventional radiography. The cut points used for progression by worsening of joint space are above what is likely to be measurement variation. The study examined osteoarthritis progression using joint space assessment and the K/L score. In a sense, the findings for the BMI effect at the knee validate the approach taken to assess incident and progressive knee osteoarthritis.
The study has some limitations, which the authors clearly acknowledge and discuss—that is, the number of participants who did not return for the follow-up evaluation, and, possibly related to this, the relatively low rates of incident and progressive osteoarthritis for a study of this duration. Although it is important to note this issue, it seems an unlikely explanation for the difference in the effect of BMI between the knee and the hip. A selective loss to follow-up may have weakened the findings related to hip osteoarthritis incidence and progression—for example, if people with rapidly worsening osteoarthritis did not come back because of greater pain or disability, or if there was a selective loss of heavier participants. However, it is difficult to see how this potential issue would specifically weaken the results detected for the hip so much more than those for the knee. It is unlikely that the loss to follow-up explains the difference in BMI effect between the hip and the knee.
Several epidemiological studies have sought to advance our understanding of the mechanism of the effect of BMI on osteoarthritis at specific joint sites. Previous studies showed little evidence of a metabolic link between body weight and knee osteoarthritis. With one exception,7 population-based studies have not shown an independent relationship of a metabolic correlate of obesity (eg, serum lipids, glucose or glucose tolerance test, body fat distribution and blood pressure) with knee osteoarthritis.8,9,10,11 As Reijman et al describe in the discussion of their paper, leptin may represent a systemic factor linking body weight and osteoarthritis, although this mechanism does not reveal why a BMI effect should be different between the hip and the knee in this study.
Both the hip and the knee withstand large mechanical loads during weight-bearing activities. However, the hip joint has the anatomical advantage. The bony shape of the hip joint provides excellent stability and places fewer demands than the knee does on the capsule, ligaments and muscles. In contrast with the hip, the situation at the knee is a bit sobering. The capsule, ligaments, menisci and muscles at the knee are often required to counteract large external loads acting on the joint. Dysfunction of any of these structures (eg, owing to osteoarthritis or injury) influences knee-joint mechanics, potentially increasing stress on the articular cartilage. Such a milieu may help to explain why the effect of excess body weight is greater at the knee.
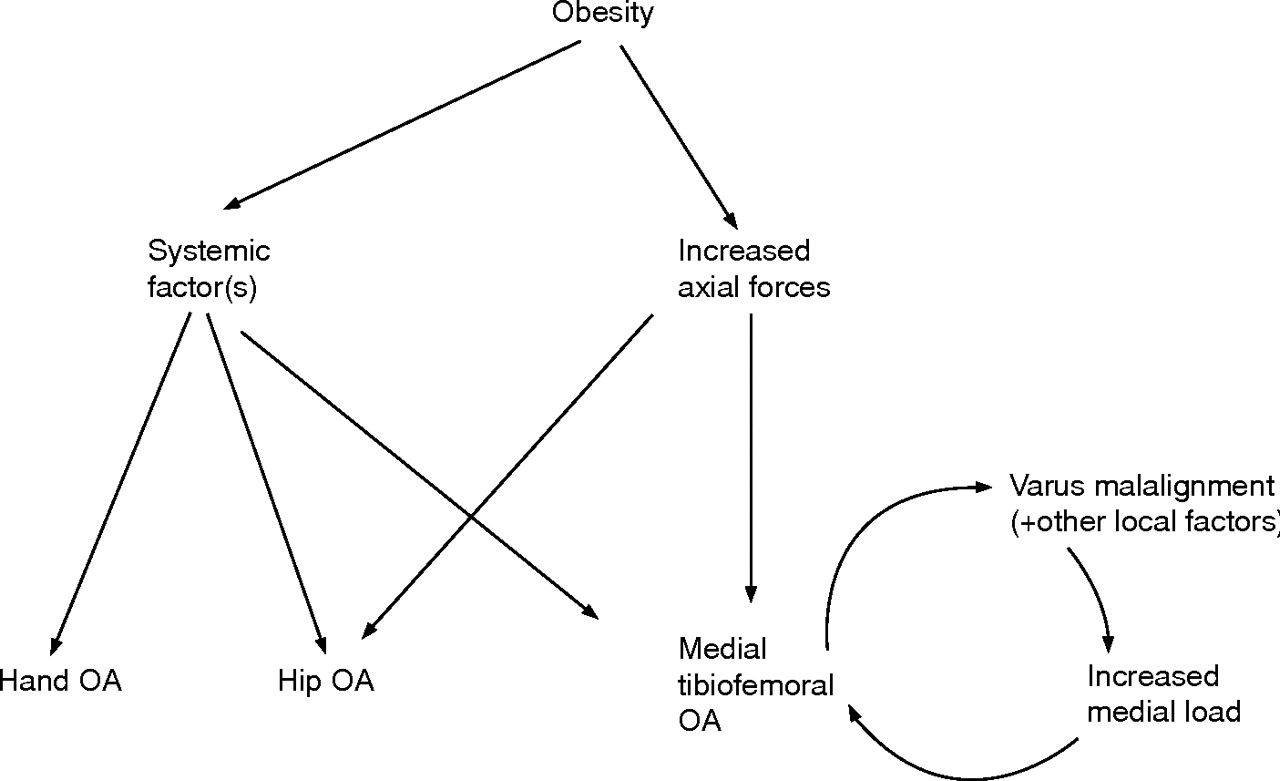
A local factor that may render the knee especially vulnerable to the effect of body-weight forces is knee malalignment. Malalignment may precede and/or be a consequence of knee osteoarthritis. Whether an original cause or effect of osteoarthritis, malalignment increases the risk of osteoarthritis disease progression. Malalignment essentially funnels in and directs body-weight forces to a specific tibiofemoral compartment. In keeping with this possibility, the relationship between BMI and osteoarthritis severity in varus knees did not persist after adjusting for the severity of malalignment, suggesting that BMI and malalignment did not act independently.12 Also, the BMI effect on progression was different in knees according to their baseline alignment category.13 In a paradigm we had previously developed12 (fig 1⇓), greater BMI may amplify and/or accelerate a cycle of medial tibiofemoral compartment cartilage loss and varus malalignment in progressive knee osteoarthritis, or accelerate a vicious cycle between a local factor other than or in addition to malalignment and knee osteoarthritis progression.12 This paradigm describes why any BMI effect could be greater at the knee than the more general effect of a systemic pathway through the leptin route on the hip and other joints.
{kind=link}
Paradigm showing possible relationships 55 between obesity and osteoarthritis at various joint sites.
The study by Reijman et al introduces some fascinating questions. This study used established and widely applied definitions of incident and progressive osteoarthritis. In their discussion, the authors rightly note that these definitions, although they have been extensively validated, are somewhat arbitrary in the continuum that is the natural course of osteoarthritis. Might the results have differed if what constitutes incident osteoarthritis and progressive osteoarthritis had been defined using other points in the radiographic steps between the healthy joint and the end-stage joint? Might the results have differed if incident osteoarthritis and progressive osteoarthritis had been defined using specialised magnetic resonance imaging protocols to assess the joint globally or joint tissues specifically, or to quantify cartilage? Such protocols have been developed for the knee, but have not been refined for the hip. There is uncertainty about whether incident and progressive osteoarthritis at the hip should be defined identically to the outcomes defined at the knee. Although the approach taken by the authors is reasonable, do the anatomy, mechanics and function of the hip require unique radiographic definitions of incident osteoarthritis and osteoarthritis progression? The authors’ ability to look at the effect of a BMI in the obese range was limited by the small number of individuals in the population whose weight fell into this category. Might obesity (ie, BMI >30) increase the risk of incident or progressive osteoarthritis at the hip? The study’s findings are compelling for overweight. Will the results differ for obesity? Might there be a subset of people in whom BMI has a stronger effect at the hip than when the population is considered as a whole?
Is it safe for people with hip osteoarthritis to gain weight? Of course, no. Reijman et al deliberately examined important questions relating to joint structure outcomes. There is little in the literature about the effect of overweight and obesity in the setting of hip arthritis on person-relevant outcomes, but reasons for people with hip osteoarthritis to avoid excess body weight are abundant. Overweight and obesity are associated with substantial morbidity to other organ systems. Also, excess body weight in the setting of hip osteoarthritis may increase the likelihood of incident disability or disability progression possibly because of direct effects, interaction between excess weight and arthritis symptoms and limitations, and interaction between excess weight and medical comorbidities.
The study by Reijman et al is an outstanding advance. In the next step, epidemiological investigators should consider applying magnetic resonance image techniques to assess specific tissue effects towards an overall goal of further enriching our knowledge of what greater BMI does to the hip and the knee, and should consider studies to elucidate the role of greater BMI in disability in people with osteoarthritis in these crucial joints.
REFERENCES
Footnotes
See linked article, p 158
Competing interests: None declared.